March 13, 2026
Developing an oncology therapy requires a series of key decisions, each with the power to move a program forward or set it back. Pipelines are increasingly crowded, and many companies are chasing the same, increasingly precise targets. A staged workflow that begins with broad in vitro and organoid screening, progresses through ex vivo tissue, and culminates in PDX models creates a clear path toward clinically relevant validation. Together, these systems support decisions that reflect real patient biology and reduce risk at every stage.
To reduce the risk in these decisions, teams need models that reflect real patient biology, not simplified systems. That is why patient-derived xenograft (PDX) models have become essential. Because they preserve the genomic, molecular, and histopathological complexity of human tumors, PDXs offer a level of clinical relevance traditional in vivo models cannot match. They help teams probe mechanism of action (MoA), refine biomarker strategies, and evaluate therapeutic response in a way that mirrors real-world disease heterogeneity.
This blog is a practical guide to where PDX models add the most value and how they help de‑risk development from early translational questions to resistance mapping.
Why Patient‑Derived Models Bridge the Lab–Clinic Gap
Drug developers today have access to an impressive spectrum of preclinical tools. Each platform can illuminate different aspects of tumor biology or therapeutic response.
But when the goal is to understand how a therapy will behave in the complexity of real human disease, PDX models rise to the top. Their defining strength is simple but profound: they preserve the architecture, diversity, and biological nuance of actual tumors.
PDX models offer several advantages that make them uniquely powerful in translational research:
- They retain the genomic, molecular, and histopathological characteristics of the original patient tumor, maintaining the features that drive therapeutic sensitivity and resistance.
- Large PDX collections capture the diversity seen in real patient populations, enabling teams to test hypotheses across a broad range of tumor types, mutational backgrounds, and disease states.
- They function as patient avatars, providing a controlled yet clinically relevant way to explore how a therapy might perform across different tumor contexts.
- Their ability to reflect real patient variability makes them a powerful tool for translational decision making, especially when refining biomarker strategies, selecting patient subgroups, or anticipating resistance.
Because of their fidelity, PDX models often can close the gap between laboratory findings and clinical outcomes. They help teams move beyond simplified systems and into models that behave like the patients they aim to treat. In doing so, PDXs provide a more reliable foundation for the decisions that shape oncology development.
A Reliable Path to Clinically Meaningful Validation
PDX models are created by engrafting patient tumor tissue into immunodeficient mice, where the tumor can grow, adapt, and be passaged while maintaining the defining characteristics of the original malignancy (Figure 1). This ability to preserve patient-specific architecture and biology is what gives PDX models their power and why they have been widely adopted across the industry.
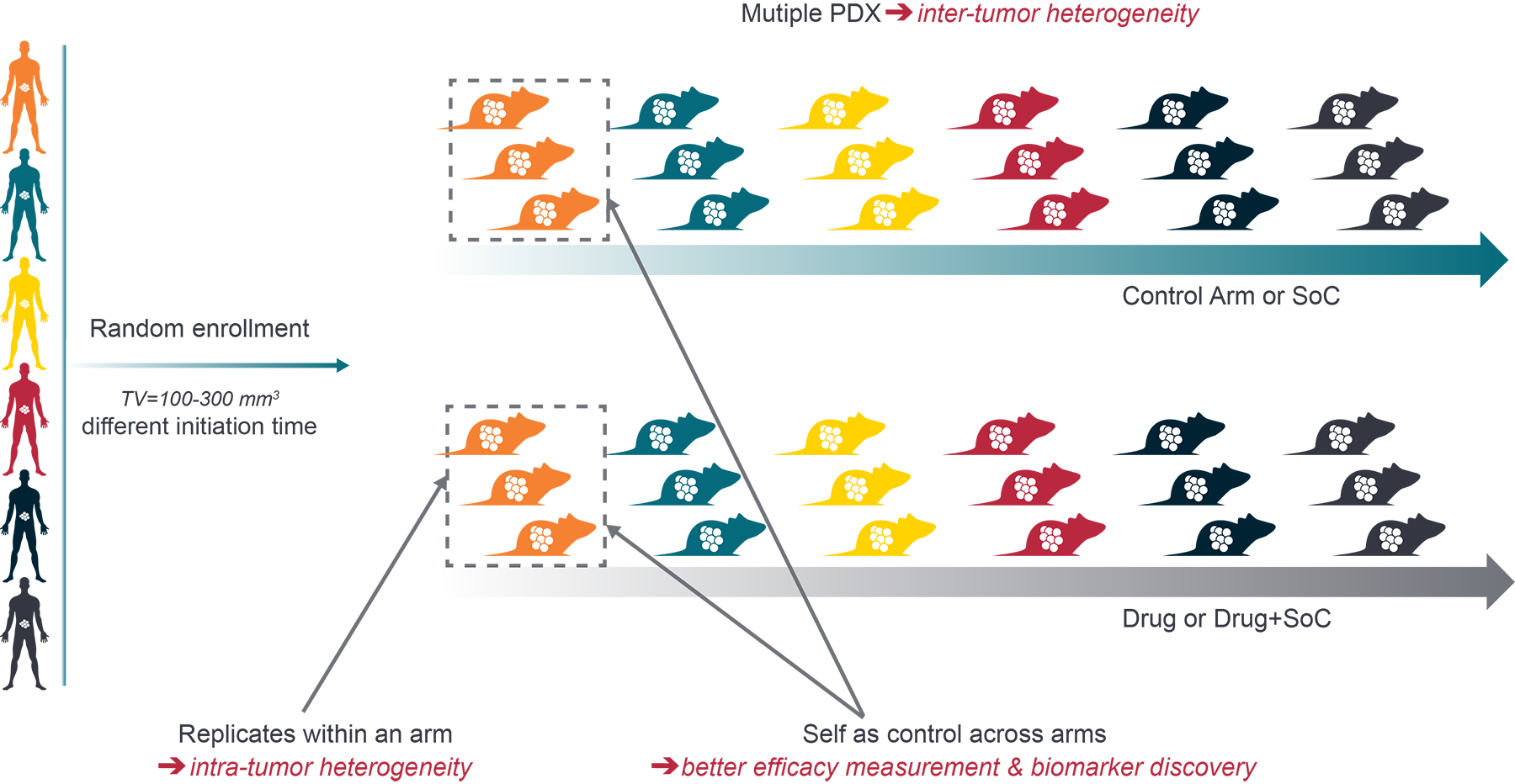
Figure 1. A representative PDX Mouse Clinical Trial Design
Over the past decade, PDX models have become a cornerstone of translational oncology, offering a level of predictive insight that traditional systems rarely achieve. They excel in:
- Drug screening and MoA studies, where biological fidelity is essential for understanding how a therapy interacts with real tumor biology
- Biomarker discovery, supported by annotated models that link molecular features to therapeutic response
- Tumor biology research, enabling teams to study growth patterns, heterogeneity, and disease evolution in a clinically relevant context
- Later stage validation, where clinical relevance outweighs throughput and teams need confidence before advancing toward the clinic.
PDXs are more resource intensive than in vitro systems. But when the goal is to make a high consequence decision, they are often the most decisive models available.
MoA Validation, Biomarkers, and Patient Stratification
Once a therapy shows early promise, the focus shifts from “does it work” to “how does it work” and “who is most likely to benefit.” PDX models become especially valuable at this point. Their biological fidelity allows teams to interrogate mechanism, refine hypotheses, and build a clearer picture of therapeutic relevance across diverse tumor backgrounds.
Key contributions of PDX studies include:
- Validation of target engagement and downstream biological effects, confirming that the therapy behaves as expected in a humanlike tumor environment
- Early support for biomarker hypotheses, using well annotated models that link molecular features to response patterns
- Identification of patient subgroups most likely to benefit, enabled by large and diverse PDX biobanks that reflect real world heterogeneity
- Integration of genomic, transcriptomic, and proteomic data, strengthening translational interpretation and supporting precision oncology strategies.
This combination of biological realism and deep molecular annotation makes PDX models one of the strongest platforms for precision oncology. They help teams move beyond broad assumptions and toward evidence-based patient selection, ultimately increasing the likelihood that a therapy will succeed where it matters most: in the clinic.
Resistance Mapping and Longitudinal PDX Studies
Modern oncology development requires anticipating resistance, not simply responding to it once it appears. As therapies become more targeted and patients receive multiple lines of treatment, the evolutionary pressure on tumors intensifies. To make confident decisions, teams now need models that reflect current standards of care, real-world treatment histories, and the resistance patterns that emerge under therapeutic pressure. Next generation PDX approaches are designed to meet this need, offering tools that more accurately mirror the clinical environment:
- Pretreated and resistant PDX models that reflect prior exposure to targeted therapies, chemotherapies, and immunotherapies, enabling teams to study how tumors adapt and which vulnerabilities remain
- Longitudinal studies and serial sampling that track tumor evolution over time, revealing the molecular and phenotypic shifts that drive resistance
- Mouse Clinical Trials (MCTs) that simulate patient populations by testing therapies across large, diverse PDX cohorts, helping identify responders, nonresponders, and emerging resistance patterns
- Insights that guide rational combination and sequencing strategies, informed by how tumors behave under different therapeutic pressures.
These next-generation approaches allow researchers to move beyond static snapshots of disease and toward a dynamic understanding of tumor evolution. By integrating resistant models, longitudinal data, and population scale in vivo studies, developers gain a clearer view of where therapies are likely to succeed, where they may falter, and how to design strategies that stay ahead of resistance rather than chasing it.
Conclusion
PDX models have become essential tools for translational oncology because they offer something few other systems can: a realistic and clinically relevant view of how therapies behave in human-like tumors. Their ability to preserve patient-specific architecture and molecular complexity allows teams to evaluate therapeutic response in a setting that mirrors real disease.
If your goal is to advance a therapy with confidence, PDX models offer a proven path forward. As programs move into later discovery and translational stages, where the stakes rise and the margin for error narrows, PDX models meaningfully reduce risk and help teams make decisions with greater confidence and clarity.
Frequently Asked Questions
On-Demand Webinar
Preclinical Drug-Resistant Tumor Models for Cancer Drug Development

Cite this Article
Baillargeon, M., (2026) - Crown Bioscience. https://blog.crownbio.com/pdx-models-de-risking-treatment-development
Related Posts