Cancer stem cells (CSC) represent one of the most challenging targets for cancer therapy today. Here we review the background to this phenomenon and explore the various experimental models that are used to investigate anticancer therapies targeting CSCs.
Cancer heterogeneity is a fact. However, over the past two decades, cancer hierarchy has emerged as a novel paradigm, transforming our vision of tumor heterogeneity and therapeutic management of cancer. Similarly to normal tissues, cancers contain a minor stem cell-like cell compartment fueling the mass generation of differentiated daughter cancer cells.
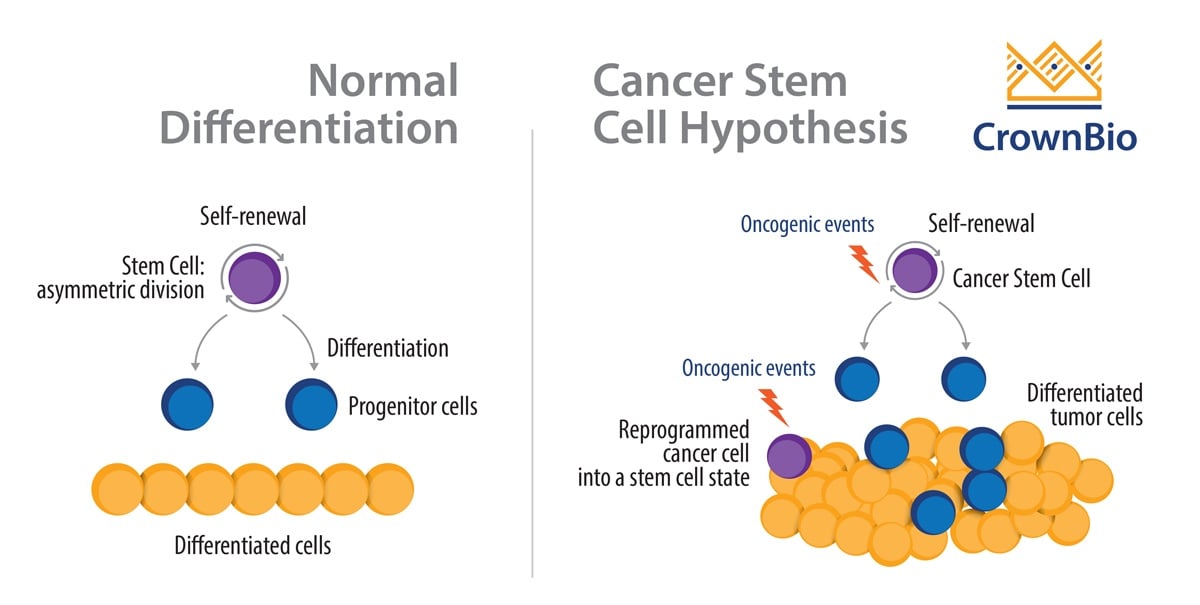
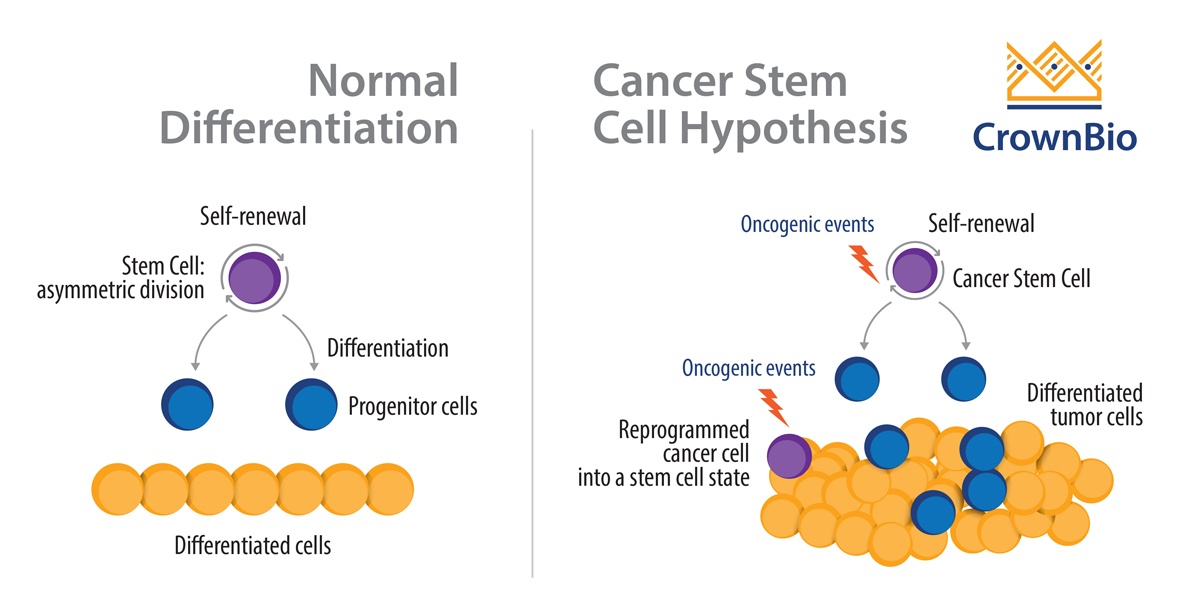
In normal cellular physiology, stem cells are defined by their ability to divide asymmetrically. Depending on their molecular and cellular environmental context, stem cells can either:
Self-renew and generate a copy of the original stem cell, or
Undergo differentiation and produce the differentiated cellular lineages of a given tissue.
Similarly, cancer stem cells (CSC) can also self-renew, as well as generate a progeny of differentiated cancer cells.
Most studies investigating CSC however, have studied tumor-initiating cells. These are cells which:
Initiate tumor formation in animal models (with this capacity being confined to CSC according to the CSC paradigm)
As well as giving rise to non-CSC by differentiation (cancer cells which lack the ability to self-renew and differentiate).
How do Cancer Stem Cells Arise?
The existence of CSC has been the subject of a highly controversial scientific debate ever since their first identification in acute myeloid leukemia (AML) back in 1997.
CSC emergence has been attributed to:
The oncogenic transformation of normal stem cells.
The dedifferentiation of mature tumor cells driven by the activation of morphogenous pathways during cancer progression.
Oncogenic Transformation of Normal Stem Cells
The best evidence for CSC originating from normal stem cells was provided by three back-to-back articles published in 2012. These studies tracked brain, colon, and skin stem cells during carcinogenesis using genetic markers. In the tissues investigated, the transformed stem cells were the cellular precursors of cancer, as well as the key cellular targets to achieve durable tumor regression.
By extension, a number of stimuli from the microenvironment can also induce activation of stem cell molecular programs in cancer cells. These include inflammation, hypoxia, TGF-beta, and chemotherapeutic pressure. The most studied stem cell pathway in cancer is perhaps the Wnt/beta-catenin pathway.
Current CSC Research and Targeting
Two decades of extensive research in this field have identified tumor-initiating cells in virtually all cancers, including melanoma, breast, colon, lung, brain, liver, AML, chronic myeloid leukemia (CML), and more.
On top of their regenerative properties, CSC are also responsible for metastasis, cancer resistance to conventional therapies (chemotherapies and radiotherapies), and cancer recurrence post-treatment.
As a result, cancer stem cells represent the ultimate, and probably most challenging, target for cancer therapies.
How to Preclinically Define Agent Efficacy on CSC
While the CSC paradigm is firmly established in hematopoietic cancers such as AML and CML, the existence of CSC in solid tumors is more of a controversial issue. Across a variety of indications, CSC are defined by specific extracellular markers which allow the identification of both CSC and non-CSC compartments. Breast and colon cancers are the best-documented indications regarding the existence of solid tumor CSC.
Cancer Stem Cell Markers
Tumor type
CSC phenotype
Reference
AML
CD34+/CD38+
Bonnet and Dick, 1997
Brain
CD133+
Sinh et al., 2004
Breast
CD44+/CD24-/low
Al-Hajj et al., 2003
Colon
CD133+
O'Brien et al., 2004
Melanoma
ABCG5+, CD20+
Shatton et al., 2008
Multiple myeloma
CD138-, CD20+
Matsui et al., 2008
Prostate
CD133+/CD44+/α1 β2+
Collins et al., 2005
Alternatively, with a lack of specific markers, a variety of functional tests can be used to define “stemness” among cancer samples. These include side population identification, ALDH assay, and the tumorsphere culture enabling anchorage-independent 3D growth.
The CSC percentage in a given sample is dependent on a number of variables. These include whether the sample was obtained after 2D or 3D in vitro growth, or in vivo growth in animal models. In addition, the degree of host immunodeficiency is also another factor which impacts the frequency of CSC in tumors. The various murine models can be:
immunocompetent (wildtype): syngeneic (relying on the engraftment of a murine cancer cell line) and primary models developed in a WT background (for which carcinogenesis is either spontaneous or induced chemically or genetically). These immunocompetent models allow you to test cancer immunotherapies.
immunodeficient (e.g. NOD-SCID, RAG-/- which lack adaptive immunity): mostly used for patient-derived xenografts (PDX) or traditional cell line derived xenograft models
severely immunodeficient (e.g. RAG-/- x γc-/-, NSGTM which lack adaptive immunity and some components of the innate immune system): again used for cell line or patient-derived xenograft models
Immunocompetent Models
Syngeneic transplants, as well oncogene and chemically-induced models, offer the most complete picture when it comes to understanding the microenvironment’s influence on cancer stemness. These models also allow the investigation of CSC targeting by immunotherapies.
One great advantage of syngeneic and cell line-derived xenograft models is the amount of published evidence regarding their hierarchy as well as their CSC phenotype. Nevertheless, syngeneic tumor models pose the problem of overextended in vitro culture that can potentially alter the heterogeneity population dynamics and the cell’s tumor initiating capacities.
In comparison to transplant models, murine primary models have multiple advantages in reflecting cancer progression, and microenvironmental changes during the various phases of the oncogenic process. On the other hand, oncogene-driven models may fail to recapitulate tumor heterogeneity and hierarchy, leaving chemically-induced or spontaneous murine tumor models as probably the best primary model option.
These chemically-induced or spontaneous murine tumor models, however, have the tendency to develop cancers which do not completely model their human cancer counterpart (e.g. methylchlorantherene (MCA)-induced sarcoma, New Zealand black mice for Chronic lymphocytic leukemia).
Finally, when considering syngeneic and primary models for cancer stem cells studies, species specificity needs to be considered. A number of cancer stem markers, such as Stem cell antigen 1 (Sca-1), are specifically confined to murine stem cell biology and therefore cannot be transposed to human cancers. This means also that their associated signaling pathways also cannot serve as therapeutic targets for human diseases.
Patient-Derived Xenografts
Patient-derived xenografts (PDX) potentially offer the most relevant options when looking for CSC therapeutics, excluding immuno-oncology drugs. PDX are never passaged in vitro and their CSC percentage, phenotype, and molecular signatures should be therefore comparable to their original parental tumor. PDX, unlike traditional xenografts, also lack any in vitro-induced or genetically engineered immortalization which might alter their CSC phenotype.
The CSC proportion in PDX samples is likely to be influenced by whether the patients were subjected to prior therapies or if the sample comes from a metastatic site. Immunotherapies also have their part to be played in PDX CSC targeting strategies with the use of humanized mice.
Conclusions
The CSC paradigm has revolutionized our understanding of tumor biology and created opportunities for novel therapeutic strategies targeting CSC. Exploring the efficacy of novel cancer therapeutics requires a range of models and tracking techniques to fully assess the potential of therapies to target CSC and achieve durable and complete eradication of tumors.
Cite this Article
TE, E., (2018) Are Cancer Stem Cells a Prime Target for Therapy? - Crown Bioscience. https://blog.crownbio.com/cancer-stem-cell-models
Why Tumor Heterogeneity Challenges Clinical Trials Tumor heterogeneity remains a major obstacle in clinical trials. Differences between tumors and eve…
Successful drug discovery requires streamlined services to manage studies, collaborations, and materials, while also minimizing logistical challenges …
Pioneering a Future of Faster, More Effective Treatments Introduction: Why AI is the Future of Pharmaceutical Innovation The landscape of drug discove…