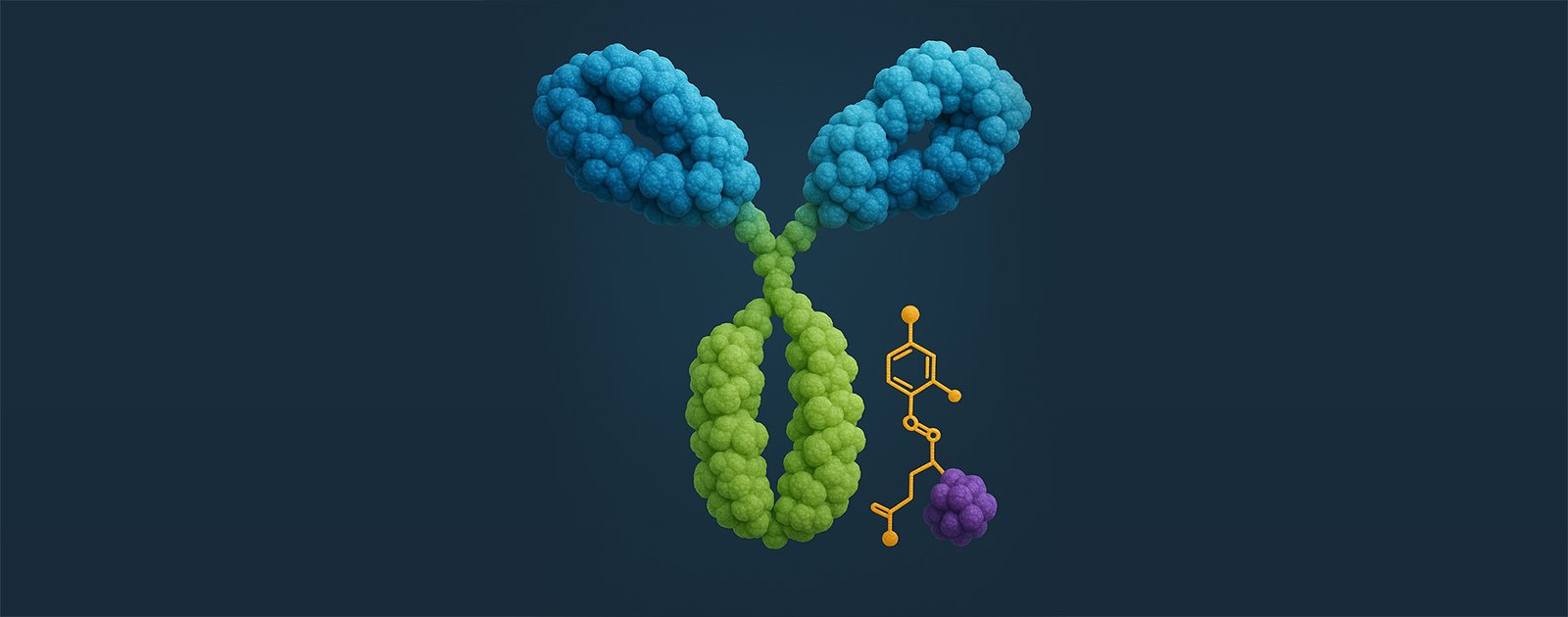
Antibody-drug conjugates (ADCs) are among the most exciting advances in target cancer therapy. They combine the specificity of monoclonal antibodies with the cytotoxic potency of small molecule drugs to focus treatment on malignant cells while reducing damage to healthy cells.
ADC toxicity is the result of different components and mechanisms of action. To fully understand the complex and multifaceted nature of this toxicity, it’s essential to examine the different ways toxicity can occur.
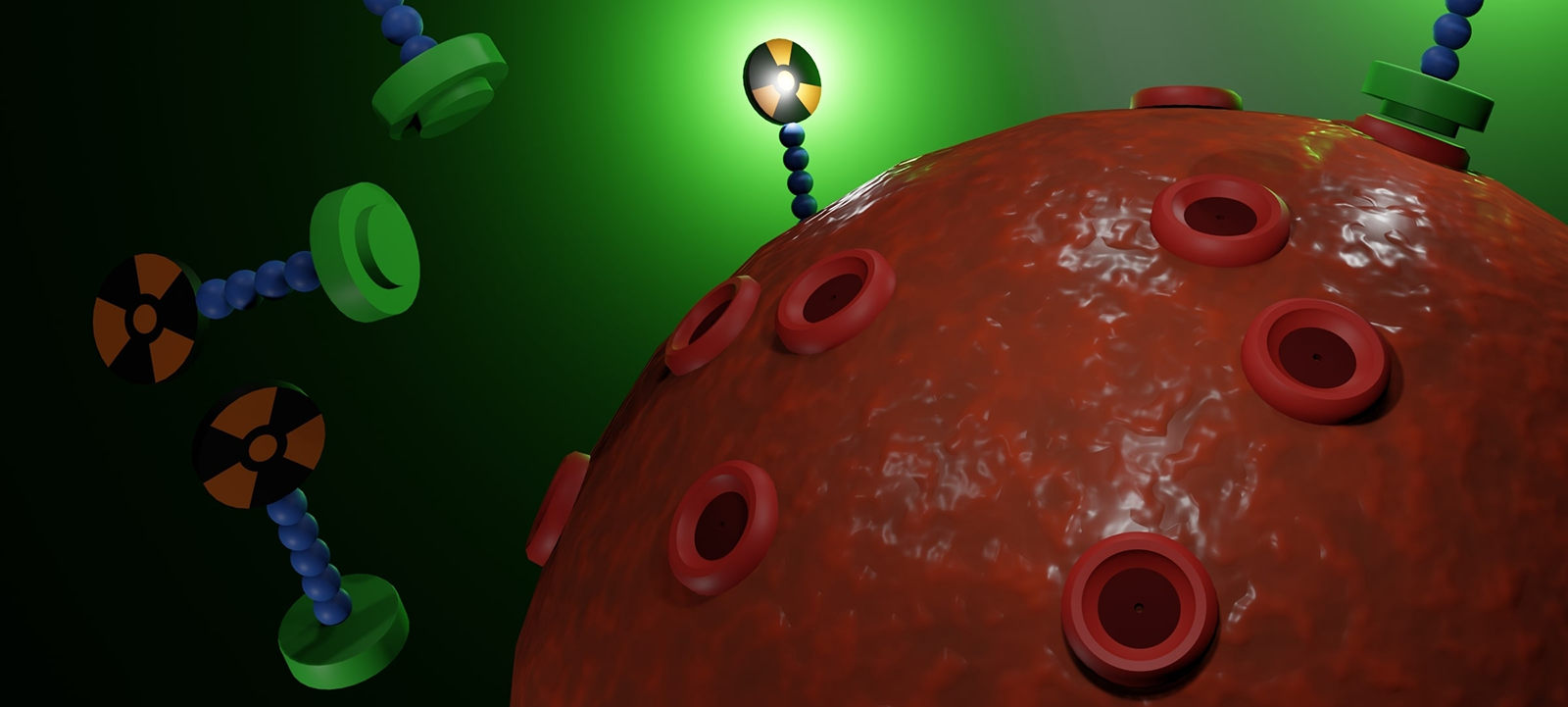
The goal of ADC development is to create a drug that correctly finds and binds to the intended site and target (on-site, on-target), thereby killing antigen-expressing cancer cells. On-site, off-target toxicity occurs when the ADC reaches the tumor location but affects nearby cells that don’t express the target antigen.
Due to the heterogeneous nature of tumors, this can result in the killing of cancer cells that don’t express the target antigen, but it can also lead to inflammation and damage in localized tissues when these nearby cells are healthy.
In contrast, non-cancerous cells in healthy organs may also express the target antigen. When the ADC binds to these cells, it can damage these healthy organs and cause side effects in patients (off-site, on-target toxicity). Here, ADC developers must concentrate on discovering new antigens that are only expressed by cancer cells, to minimize ADC binding in healthy tissues.
They can be harder to predict and manage, potentially causing unexpected tissue damage. Crucially, they can impact vital organs or bone marrow, which can leave patients vulnerable to infections and may require treatment to be stopped completely.
Thrombocytopenia: Among the most common dose-limiting toxicities seen with ADCs, a reduction in platelet count can result from ADCs utilizing microtubule inhibitors or DNA-damaging agents as megakaryocytes (or their precursors in the bone marrow) can be affected.
Neutropenia: A reduction in neutrophils (a type of white blood cells) frequently accompanies ADC therapies as neutrophil precursors are sensitive to cytotoxic payloads. This toxicity is of particular concern as it increases the risk of serious infection.
Peripheral neuropathy: A toxicity commonly associated with ADCs utilizing microtubule inhibitors, which is likely the result of non-specific uptake of ADCs or free payload by peripheral neurons.
Ocular toxicity: Blurred vision, dry eyes, and keratitis are a significant adverse event associated with several ADCs. This may be the result of the expression of target antigens in ocular tissues or the accumulation of hydrophobic payloads in the vascularized tissues of the eye.
Advanced models, such as the organoids and patient-derived xenografts (PDXs), provide highly translational platforms to assess toxicity and are quickly becoming the gold-standard for preclinical therapeutic development.
Organoids offer a controlled, three-dimensional environment that is more physiologically relevant than traditional two-dimensional cell cultures, allowing developers to isolate and analyze the individual mechanisms and components that play a role in ADC functionality, thereby identifying and overcoming the reasons for toxicity.
Additionally, as they preserve the architecture and natural heterogeneity of tumors, they enable developers to understand how tumor architecture affects the distribution and penetration of ADCs within cells, as well as the rate of uptake. For example, as they maintain the target expression patterns seen in tumors, they allow research teams to identify and mitigate on-target toxicity that may occur when normal tissues express the same target as a tumor.
PDX models are particularly useful as they retain not only the diversity and architecture of tumors, but also reflect aspects of the stromal, vascular, extracellular, and immune components seen in human tissues, to better reflect how ADCs behave in real patients. For example, they can reveal how ADCs are processed and metabolized by patients, and how dosing and scheduling can be optimized to find the optimal balance between efficacy and toxicity.
To aid research teams looking to optimize payloads, Crown Bioscience utilizes site-specific conjugation techniques, along with bioconjugation, physicochemical characterization, DAR, and endotoxin testing. Mass spectrometry analysis is also available to precisely assess pharmacokinetics (PK) and drug-to-antibody ratio (DAR), providing reliable data for informed decision-making in development.
Modifying antibodies
Antibody engineering is another promising approach to reducing ADC toxicity. This includes the development of bispecific antibodies which require dual-antigen binding before they activate, affinity modulation to optimize tumor targeting while minimizing on-target/off-tumor effects, and Fc engineering to reduce immune-mediated toxicity.
Comprehensive antibody-generation services, allow developers to design and produce antigens; generate hybridomas; screen antibodies for binding, ADCC, and internalization; and complete deep-phase screening to optimize leads. Additionally, where small-molecule integration is offered, the therapeutic potential of ADCs is enhanced, expanding the options for optimized ADC strategies.
To find out more about how integrated preclinical solutions are accelerating the development of bispecific antibodies, read our white paper.
Optimizing dosing regimens
Modifying clinical dosing schedules has proven to improve the therapeutic index of ADCs in clinical settings and it is PDX models, that can unlock a detailed evaluation of these different dosing regimens in the preclinical setting. PDX models allow research teams to investigate how fractionated dosing can improve tolerability, extended dosing intervals allow for recovery from reversible toxicities, and combination therapies may support dose reduction.
Employing inverse targeting strategies
Inverse targeting represents an exciting new advance in ADC development. It involves administering payload-binding antibody fragments along with ADCs so that the released payload is binded, neutralized and cleared from plasma to decrease the exposure in non-tumor tissues. In vitro cell cultures and in vivo AML animal models have been central to the development of this innovative approach which has the potential to substantially reduce off-target ADC toxicity.
Conclusion
Off-target toxicity remains a significant challenge in ADC development. However, advanced preclinical models and techniques offer research teams the tools they need to navigate the challenge of ADC toxicity successfully, helping them accelerate the development of safer, more effective ADCs that fulfill the promise of this transformative therapy.
Highly targeted antibody-drug conjugates (ADCs) combine an antibody with a cytotoxic payload, covalently attached via a chemical linker. These “biolog…
Antibody-drug conjugates (ADCs) represent a cutting-edge advance in cancer therapy. These targeted agents combine a monoclonal antibody and a cytotoxi…
Introduction to Theranostics: Bridging Imaging and Therapy The convergence of diagnostics and therapeutics—collectively termed theranostics—is revolut…