Drug attrition rates for anticancer agents are much higher than in other therapeutic categories. Only an estimated 5% reach the clinical stage, which has been attributed in part to the poor translatability of preclinical data.
The pharmaceutical industry has traditionally relied on 2D cancer cell lines for in vitro anticancer drug screens. Although this system is relevant for many uses, it is recognized that there is a limited correlation between preclinical and clinical outcomes. More advanced preclinical models are immediately needed, starting at the earliest steps of drug discovery (i.e., high throughput drug screening [HTS]) to better recapitulate the complexities of human cancer, allowing for better decisions earlier. Patient-derived organoids (PDOs) and patient-derived xenograft (PDX)–derived organoids (PDXOs) have emerged as in vitro representations of tumor biology, serving as valuable tools to generate biobanks that cover a wide range of cancer indications, subtypes and genetic backgrounds.
This blog post highlights the value of highly clinically relevant, patient-relevant tumor organoids for HTS. They are superior models with better translatability and predictivity. Additionally, a case study is presented to showcase the capabilities of an assay-ready (AR) organoid platform, which offers several advantages:
Significantly reduces timelines,
Enables repeated assays with a single batch of organoids, and
Is suitable for HTS and extensive panel assessments.
The Value of Tumor Organoids
As explained, tumor organoids are 3D in vitro models that highly recapitulate the phenotypic, genomic, and morphologic (3D architecture) features of the primary tumor, all of which are important factors that can influence drug response. They are scalable, have high clinical predictivity, and are genetically and phenotypically stable even after long-term culturing and cryopreservation.
Tumor organoids developed using Hubrecht organoid technology (HUB) protocols have a preserved cancer stem cell component and thus can be propagated over long periods and even cryopreserved for follow-up studies while predictably retaining the phenotypic and genetic features of the parental tumor over multiple generations, including structural, cellular heterogeneity and somatic mutations.
Tumor organoids can be derived directly from patient tumor tissue (PDOs) or from PDXs (PDXOs), with the latter being commercially available in large, validated, and annotated collections with several key features:
Capture patient population heterogeneity, including diverse genetic backgrounds;
PDXs and PDXOs are biologically equivalent and can serve as patient avatars. Thus, they represent an alternative to primary patient cells. Both models are developed exclusively using HUB protocols and generate ample new opportunities for cancer drug discovery.
Large organoid panels leverage many patient-relevant models at the same time. This represents a revolutionary approach to early drug discovery: a tailored PDO/PDXO selection allows for a “clinical trial in a dish”. Such collections reflect patient characteristics at not only the individual-patient but also the patient-population level. Interpatient and intratumor heterogeneity are believed to be the basis for the drug resistance often seen in the clinical setting. Compounds can be screened simultaneously on a large group of models, enabling quicker decision-making about which lead compound to progress. Using large organoid panels in drug discovery and combining with biomarker analysis allows for identifying responsive cancer subtypes and genotypes, allowing early patient stratification.
Case Study: Pan-cancer 'Assay-ready' Organoid Drug Screening with Robust, Reproducible, and Clinically-relevant Output
This study compared the performance of biobanked (cryopreserved) PDXOs (the AR organoid platform) to freshly prepared patient-derived tumor organoids (the classic method).
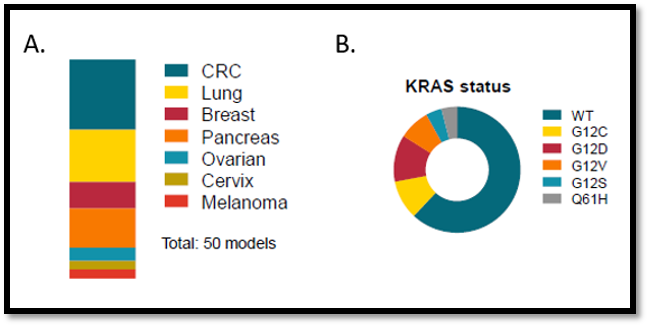
The AR platform was represented by 50 PDO/PDXO models selected from seven tumor types (colorectal, breast, lung, pancreatic, ovarian, cervix, and melanoma), and harbored several (paired) healthy tissue (control) samples (Figure 1A). The goal was to generate a heterogenous group that would be representative of the large variability in subtypes and driver mutations, illustrated by the variety of KRAS mutations across the samples (Figure 1B). Fourteen models were prepared using the classic method, also representing a range of tumor indications (not shown). To enhance consistency, all procedures were standardized, and automated liquid handling equipment was used.
Figure 1: (A) Tumor types represented in the 50 PDXO AR organoid platform and (B) KRAS mutational status across the PDXO
Proliferation and drug responses of PDO/PDXO models tested with both methods were evaluated. Organoid performance was assessed through repeated drug sensitivity testing, assessing intra- and interplate variability, CV, Z-factor, assay windows, and IC50 values. Organoid drug responses were acquired using both cell titer glo (CTG, relative cell viability to control) and high-content imaging (HCI) read-outs (average number of nuclei per organoid, relative to control).
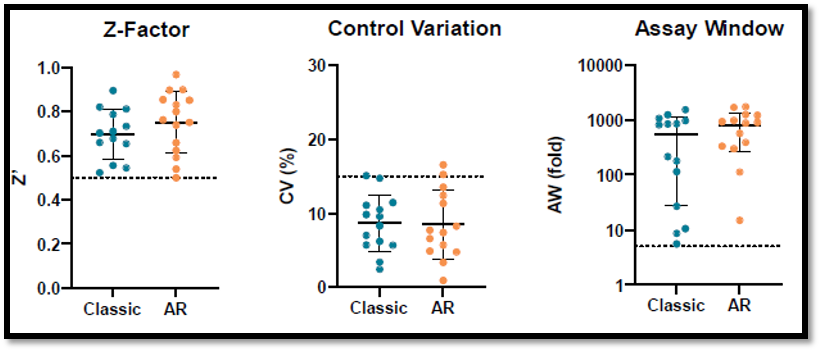
Fourteen organoid models representing all tumor indications included in the AR organoid platform were first compared for assay performance in a CTG-based drug screen assay. Overall, the classic and AR models showed highly reproducible performance, with similarly high Z-factors, low intra- and interplate control variability (CV) (<15%), and large assay windows (negative control/positive control) (Figure 2). The AR platform significantly reduced cost and shortened project timelines from months to weeks (>6-fold) from kick-off to data delivery, compared to the classic models (data not shown).
Figure 2: Comparison of AR organoid platform versus the classic method
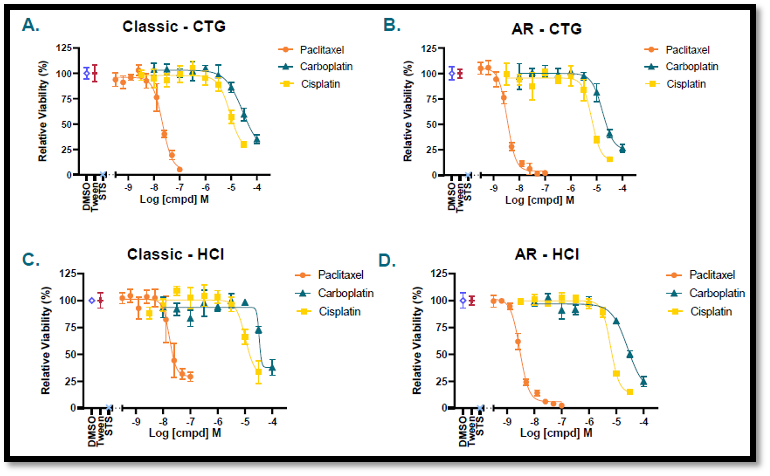
The AR platform and classic method delivered similar results in CTG and HCI assays. Figure 3 shows representative plots comparing the drug response to paclitaxel, carboplatin, and cisplatin, grown via the classic method (3A and 3C) and the AR platform (3B and 3D).
Figure 3: Drug response comparison of AR organoid platform versus the classic method(n = 4 for all assays; data normalized against vehicle control)
As shown in Table 1, highly similar IC50 (µM) values were obtained for a tested ovarian organoid model (OV5296B) prepared using the classic and AR methods. The variable slope (four-parameter) fitting in GraphPad prism shows comparable data between the two methods and CTG and HCI assays. This similarity was verified for an additional 23 models, covering a subset of seven indications with diverse genetic backgrounds (data not shown). Both platforms yielded consistent IC50 outputs, even when assays were executed months apart or at different Crown Bioscience sites. (data not shown).
Table 1: IC50 (uM) values for the classic and AR models and CTG and HCI methods
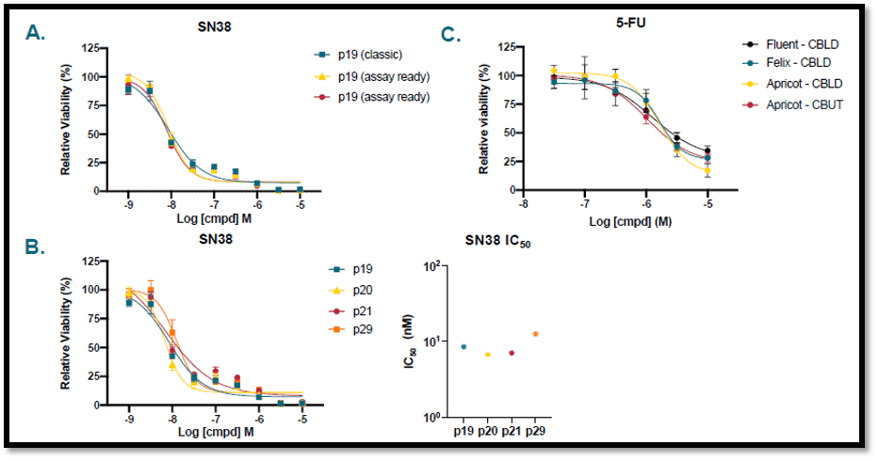
The colorectal tumor PDXO (CR5043B) model—comparing the classic and AR method—was assessed for SN38 drug sensitivity in experiments over several weeks (CTG assay, n = 4) (Figure 4A). CR5043B was propagated using the classic method for over 10 passages and tested at four different passages (p19, p20, p21, p29) for drug response . The drug response curves showed high overlap, indicating similar IC50 values (CTG assay, n = 4) (Figure 4B).
AR colorectal tumor organoids (P18T) were seeded using different liquid handling systems and at different locations (Crown Bioscience Leiden and Utrecht). The drug response to 5-fluorouracil (5-FU) was determined using HCI analysis (n = 4). The similarity in curve shape and position across these experiments highlights the interexperimental reproducibility of the results (Figure 4C).
Figure 4: Drug sensitivity of AR organoid platform and the classic method across different assays
Overall, both systems performed well. However, the AR organoid platform can significantly reduce timelines and associated costs for customers, minimizing logistical challenges and enabling screening of large tumor organoid panels simultaneously. This case study highlights that the AR platform effectively allows for distinction between sensitive, partially sensitive, and insensitive models, demonstrating organoids’ capability to enable patient stratification.
Conclusion
The cancer drug discovery paradigm is costly, risky, slow, and inefficient. Better models that are more clinically relevant and amenable to HTS can revolutionize drug discovery.
Patient-derived organoids are an in vitro platform with enhanced patient relevance compared to traditional 2D cell culture systems commonly used in HTS. Preclinical drug screening using patient derived organoids prior to in vivo assessment provides a fast, scalable and translational platform, as these 3D in vitro tumor models faithfully recapitulate the genomic, morphological, and pathophysiological characteristics of the original tumor. Furthermore, they have proven to be genetically and phenotypically stable even after long-term culturing and cryopreservation.
Implementing an organoid-based HTS requires several key components that come together to form a platform that can maximize the chances of selecting drug candidates with high translatability and clinical success. Furthermore, an AR organoid platform can save significant time and money. As the majority of available PDO/PDXO models are also available as PDXs, researchers have direct access to responsive in vivo matched models that can be used complementarily to allow for an efficient transition from early in vitro studies to late-phase animal-based validation trials.
Take your cancer drug discovery to the next level with our Organoid Models Database. With better translatability and predictivity, these organoids offer significant advantages, including reduced timelines, repeated assays with a single batch, and suitability for high-throughput drug screening. Visit our Organoid Models Database now and unlock the potential of tumor organoids for your research.
Imagine standing on the brink of a breakthrough in cancer treatment, only to be halted by one daunting barrier: drug resistance. In this episode of Cr…
Oncology drug approvals in H1 2025 In the first half of 2025, the FDA’s Center for Drug Evaluation and Research (CDER) approved a total of 16 novel dr…
Often referred to as “magic bullets” or “biological missiles”, antibody-drug conjugates (ADCs) are one of the most promising advances in targeted canc…