Patient-derived xenograft models (PDX) support more predictive, clinically-representative in vivo oncology studies than were previously accessible to researchers. Here’s how PDX models differ from traditional xenografts, and how we develop and characterize them for oncology and immuno-oncology studies.
Conventional cell line xenograft models (CDX) were routinely used in cancer research and drug discovery for many years. They are derived from immortalized cell lines, which are grown in vitro and implanted into immunodeficient mice. These traditional xenografts provide an excellent tool for early in vivo drug discovery, such as pharmacological testing. Activity information from in vitro studies can be assessed in vivo in the context of host determined factors, such as ADME and pharmacokinetics.
While cell line-derived xenografts are useful for early stage drug development, they do have their drawbacks. Adaptation to tissue culture changes the cell lines, potentially compromising clinical relevance. The selection pressure imposed by culturing cells on plastic results in the outgrowth of clones of cells that are no longer representative of the original specimen - the cell lines drift from the original disease. They also do not capture the true heterogeneity of the human clinical oncology population.
Because of their temporal proximity to the patient, and having never been subjected to the selection pressures of cell culture, PDX models closely recapitulate patient disease. They show high fidelity in histological presentation of the patient’s cancer and in its response to standard of care and experimental agents such as chemotherapy, radiotherapy, and targeted therapies.
Moreover, one major challenge when developing new targeted agents is preclinically replicating the resistance genotypes and wide range of mutation patterns seen in the clinical population. PDX models have the proven ability to replicate these characteristics.
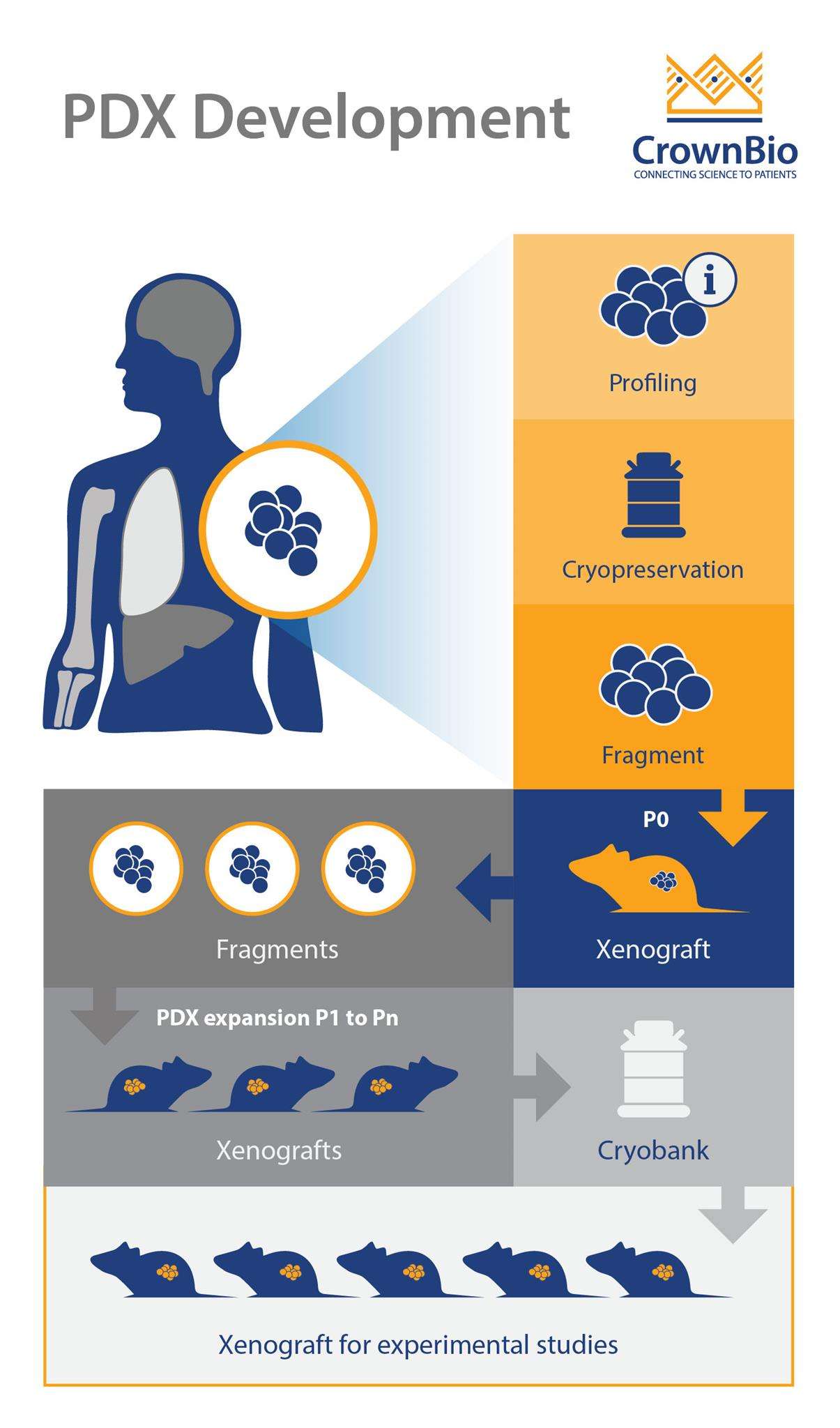
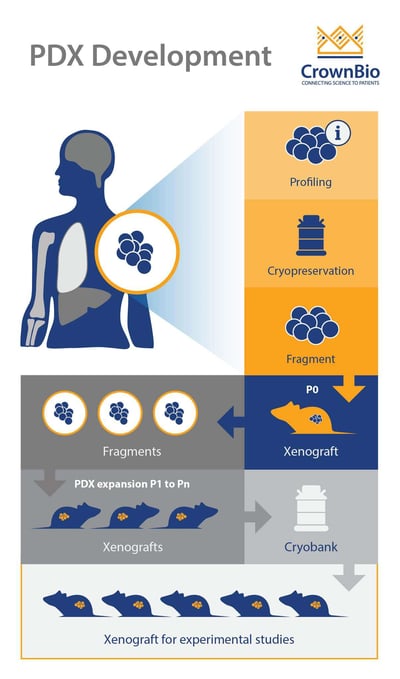
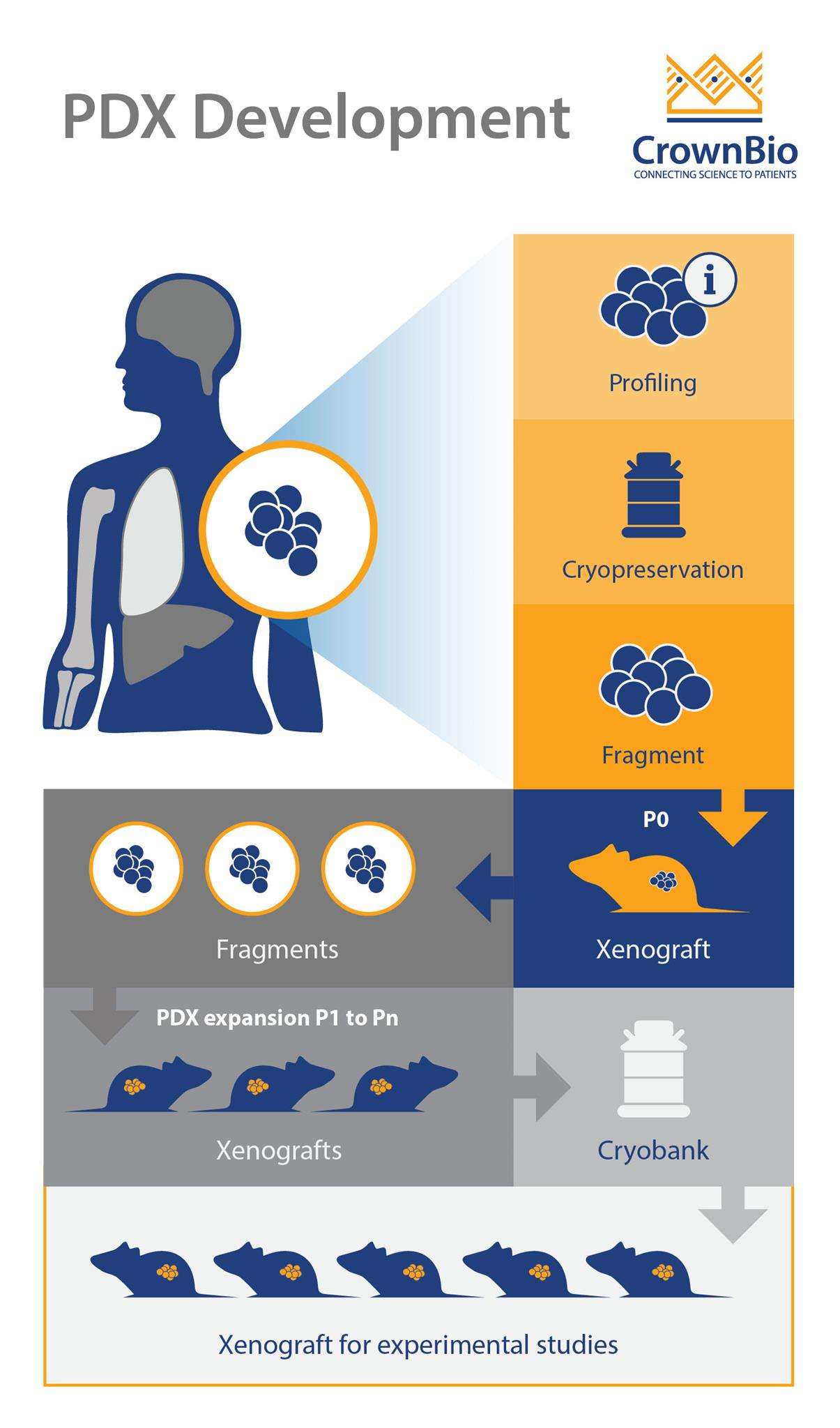
For the first implantation, patient-derived tumors may be implanted into immunodeficient mice either in the form of small tumor fragments or as tumor slurries derived from the blood of patients. The principal determinants of successful tumor engraftment into immunodeficient mice are the viability and sterility of the human tumor.
The time required to establish a PDX model varies by tumor type and grade. It can take anywhere from months to more than one year to finally get a model established. The first passage is the most difficult; if the tumor successfully grows, it will likely continue to grow in successive passages.
PDX can be implanted subcutaneously or orthotopically. PDX models are commonly established at subcutaneous sites, as cell implantation methods are easier and allow accurate monitoring of tumor size.
Orthotopically-implanted tumor cells have been shown to better mimic the drug response, growth patterns, and metastatic features of corresponding patient tumors, likely because of critical influence by the local stroma. Orthotopic implantation is more technically challenging and time-consuming, however, and often requires imaging (e.g. ultrasound, CT scan, etc.) or exploratory laparotomies to confirm the presence of internal tumors.
Validating PDX Models
One of the main laboratory management challenges with PDX models is drift from the original patient material. In order to ensure that the model is consistent during passages and over time, stringent validation and quality control is important. This is usually performed via:
Pathology QC to confirm cancer type and to compare each PDX tumor to the original patient sample.
Genetic fingerprinting via STR genotyping.
Monitoring robust and consistent growth over multiple passages.
Humanized PDX Models in Immuno-Oncology
Humanized PDX models pair human tumors within a human immune system, more accurately reflecting human immunity and pathology. Researchers can use these models to assess the efficacy of immunotherapies (or combination immunotherapy regimens). There are different ways to create humanized PDX models, and humanized mice are available from a range of vendors which support engraftment and growth of PDX models.
The most common method for the generation of humanized mice is to transplant CD34-positive human hematopoietic stem cells (HSCs), isolated from the umbilical cord blood, into immunodeficient mice.
Humanized PDX models support multiple applications, including combination therapy studies with human-specific antibodies and immune targets, or evaluation of diversity across a population.
Cite this Article
Bourré, L., (2018) The Establishment and Characterization of PDX Models - Crown Bioscience. https://blog.crownbio.com/patient-derived-xenograft-development
Advancements in oncology are increasingly driven by the ability to extract more detailed and precise information from patient tumor samples. Tradition…
Oncology continues to be a rapidly changing field with scientific discoveries transforming patient treatment and care. As it stands today, advancement…
Cancer research has evolved significantly over the years, driven by the need for more precise and efficient methods to study tumor biology, identify b…