How to develop predictive cancer biomarkers: Explore the different types and classes of cancer biomarker, and the key steps of predictive cancer biomarker development.
Advances in technology coupled with an increased interest in individualized therapies have led to the rapid expansion of precision medicine in oncology over the last few years. Precision medicine uses biomarkers to determine an optimal treatment strategy (using a targeted therapy) and assesses treatment efficacy and/or disease progression in patients.
Precision medicine approaches have fueled strategies leading to improvements in drug efficacy and patient safety, while also reducing the attrition rate of anticancer agents. The Personalized Medicine Coalition states that personalized medicines accounted for 42% of all US FDA drug approvals in 2018, and this is expected to increase over time.
Precision approaches are not a new concept - blood typing, for instance, has been used for decades. However, recent years have witnessed transformational advancements in computational power and algorithms, as well as breakthroughs in genomic technologies including next-generation sequencing (NGS) and other “-omic” signatures (e.g. proteomic and metabolomic).
Enabling Precision Medicine by Developing Cancer Biomarkers and Companion Diagnostics
These major advancements are enabling systems biology approaches that are generating novel opportunities in the field of precision medicine. This includes cancer biomarker discovery and validation strategies to identify promising candidate therapies at an early stage. The overall goal is to tailor novel therapeutics for specific patient populations and cancer indications.
Successful precision medicine strategies require two components:
A targeted therapy
A companion diagnostic (CDx) to confirm the presence of relevant biomarkers, such as genetic mutations, proteins, or other signatures.
In addition to predicting treatment response, the clinical benefits of combining these two components extend to diagnosing disease and assessing treatment effectiveness or disease progression.
Creating a biomarker strategy early in drug development offers the best opportunity for selecting optimal targets and models for the preclinical stage. Using those targets can enhance the probability that preclinical biomarkers will translate to the clinic, to improve trial and patient outcomes. An early biomarker strategy also offers ample opportunity to develop a CDx, which will be required for such translation.
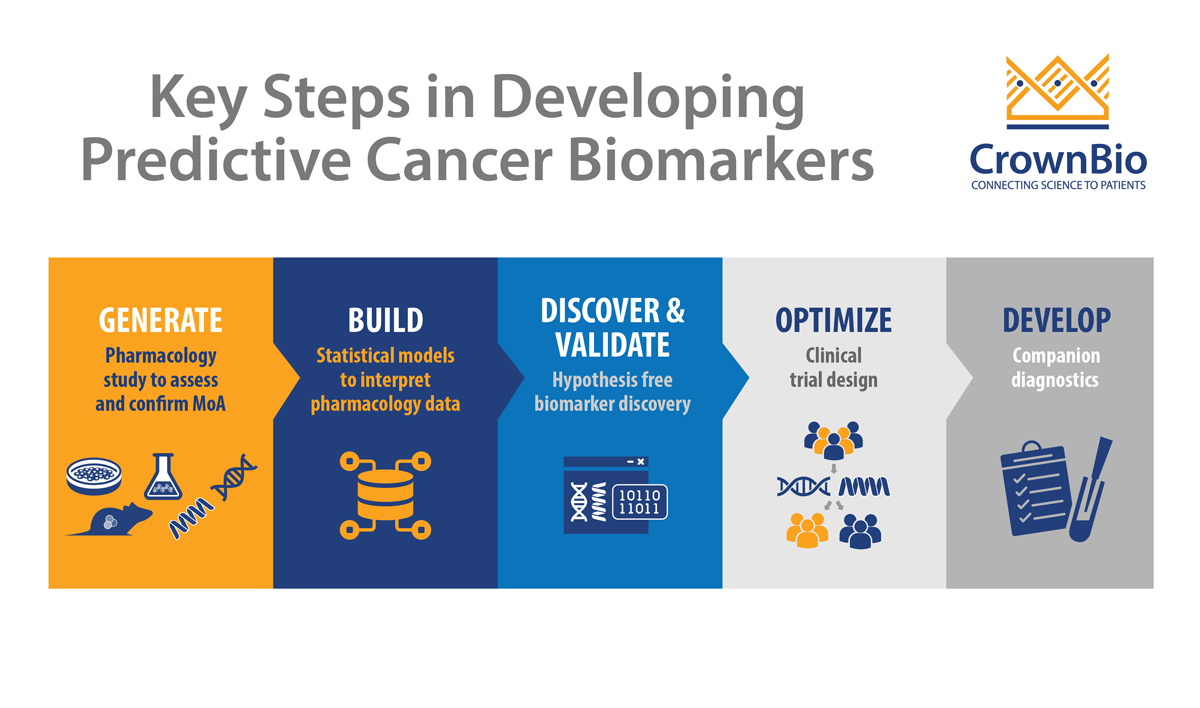
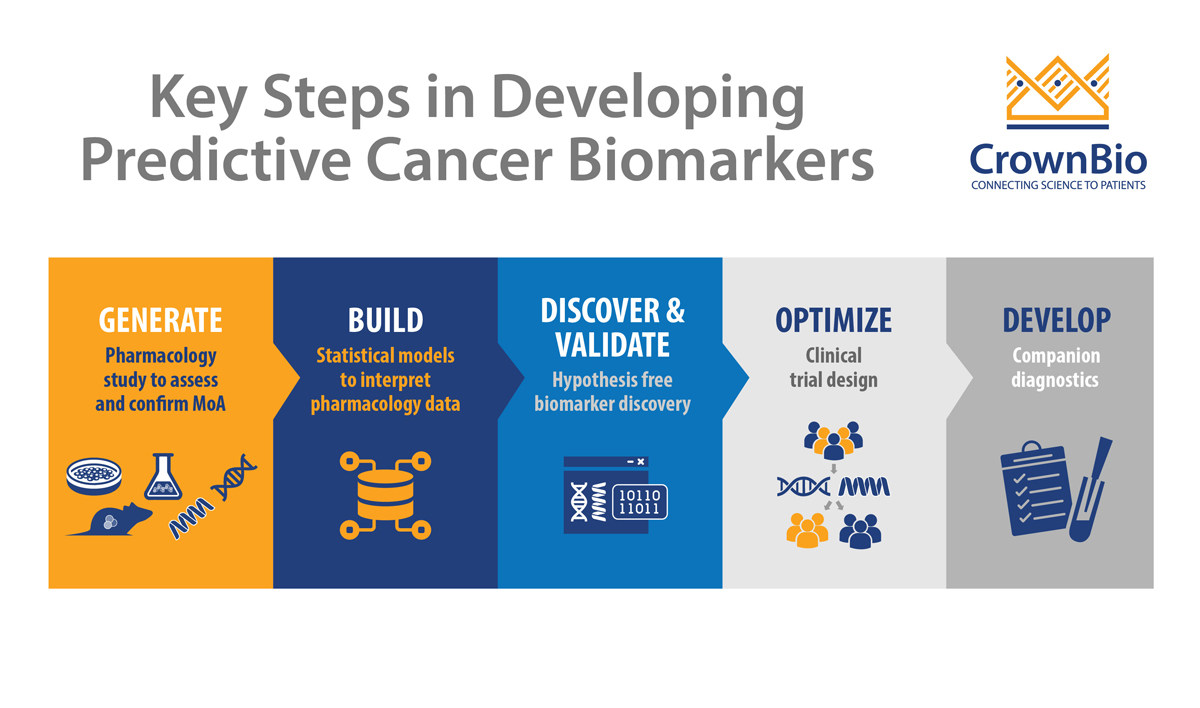
While cancer biomarker development presents many challenges, there are key steps that should be taken into account to provide the best opportunity to bridge the chasm between initial biomarker discovery studies and their clinical translation. In this post, we explore the different types and classes of biomarker which can be developed, and the key steps in predictive cancer biomarker development.
Diagnostic biomarkers: To detect or confirm the presence of a specific disease or condition.
Predictive biomarkers: To guide treatment decisions by indicating the probable effect of a specific therapy on a patient. These biomarkers identify individuals who are more likely to experience a positive or negative effect.
Prognostic biomarkers: To inform about the increased or decreased likelihood of clinical outcomes, such as disease recurrence or progression.
Different Classes of Cancer Biomarkers
There are a wide variety of potential biomarkers relevant to cancer drug development. These are often assessed by measuring levels of proteins, peptides, DNA, RNA, or other biomolecules. As discussed in an earlier post, the different types and classes of cancer biomarkers can be broadly classified as follows:
Genetic biomarkers are DNA sequences associated with an increased or decreased risk for developing a disease. This class of biomarkers can be used for cancer diagnosis and prognosis and predicting response to treatment.
Epigenetic biomarkers are indicative of altered gene functions that do not involve changes in DNA sequences. This class of biomarkers commonly includes changes in the DNA methylation status and chromatin modifications.
Transcriptomic biomarkers are derived from the global measurement of mRNA expression (i.e. transcriptomics). This class of biomarkers provides both measurements of single gene activity and a tissue-specific deeper understanding of cancer molecular subtypes.
Proteomic biomarkers provide key information about proteins, including functionality, post‐translational modifications, interaction with other biological molecules, and response to environmental factors. Advances in mass spectrometry have enabled proteomic workflows that allow for profiling large datasets with very high precision and resolution.
Metabolomic biomarkers are particularly promising because an altered metabolism is considered a hallmark of cancer. This class of biomarkers can delineate the mechanisms of metabolic pathway changes to facilitate earlier cancer detection and also predict drug responsiveness and contribute to novel therapeutic strategies.
Developing Predictive Cancer Biomarkers
Predictive cancer biomarkers are key to accurately stratifying patients who are most likely to benefit from a targeted therapy, from a safety or efficacy perspective. In addition, trials that incorporate a biomarker strategy have shown higher overall success probabilities than trials without biomarkers.
Despite the advancements in technology and value of biomarkers, there are challenges associated with translation to the clinic. Therefore, it’s important to integrate a biomarker strategy early in the drug development process, which should include a robust biomarker development method to increase the chances of success. We’ve summarized a list of the key steps to consider when developing a predictive cancer biomarker.
Biomarker Discovery
This first step entails exploratory studies and/or retrospective analyses to identify potentially useful biomarkers. Biomarker discovery involves the comprehensive molecular characterization of the clinical outcome of interest, as assessed by an established clinical endpoint. In general, for predictive biomarkers, the endpoint of interest is improved overall survival following treatment with the drug.
The discovery of a biomarker with clinical utility is possible during the preclinical stage by using experimental systems, such as:
In vitro models using a 2D cellular or 3D patient-derived xenograft organoid (PDXO) screen and/or
In vivomouse clinical trial (MCT) patient-derived xenograft (PDX) models in both in vivo and in vitro experimental systems.
In particular, individual PDX(O) models with well-defined genetic profiles can be very informative about a drug’s mechanism of action.
The key factors for success are
Commitment to biomarker discovery at an early stage
Access to a wide number/range of PDXs, with available molecular characterization and that replicate clinical diversity
Appropriate selection of PDX(O) models based on molecular data and/or a biomarker hypothesis generated using in vitro data.
Assay Development and Analytical Validation
The second step is assay development to objectively measure the biomarker. This is followed by analytical validation to assure that the assay meets acceptable standards of performance in sensitivity, selectivity, precision, accuracy, and reproducibility. It is important to note that this validates its technical performance but not its usefulness.
Clinical Validation and Utility
The final step is assessing clinical validity and utility via an analytically validated assay during a clinical trial, with multiple design options depending on the intended use of the test and availability of specimens from previous clinical trials.
Clinical validity relates to the observation that the predictive assay reliably divides the patient population(s) of interest into distinct groups with divergent expected outcomes to a specific treatment. Simply, this means that the biomarker, through its test, should be able to predict or measure the relevant clinical outcome in pretreatment samples from patients treated with a specific therapy. For example, the PD-L1 immunohistochemistry test is an approved companion diagnostic to pembrolizumab for non-small-cell lung carcinoma (NSCLC) and was used to determine clinical trial eligibility.
One of the most common reasons why biomarkers fail clinical validation is bias or systematic error that is unrelated to clinical outcomes and not reproducible. Sources of bias may include:
Differences in relevant demographic characteristics
Differences in pre-analytic variables (e.g. sample handling, storage time)
Divergence from assay protocols.
Clinical utility is a measure of whether clinical use of the test improves patient outcomes for a specific indication (that is, the final test results support specific decisions/actions that lead to an improvement of patient overall survival beyond the current standard of care). For example, two different clinical trials supported PD-L1 immunohistochemistry tests in NSCLC tissue as a companion diagnostic to pembrolizumab and nivolumab.
Likewise, there are challenges associated with clinical utility. Observational data alone is not acceptable for gene variants associated with complex disorders. Rather, determining whether a test has adequate predictive value for clinical use requires controlled comparisons with alternative test options.
Clinical Implications
There are three key issues associated with implementing a biomarker test in the clinic:
Regulatory authorities’ approval
Acceptability to physicians and patients
Impact on the cost-effectiveness of anticancer treatments.
Addressing these issues is essential.
Understanding the regulatory process is important in developing a predictive cancer biomarker. If an assay is developed as an in vitro diagnostic, then the FDA must approve it. For a laboratory-developed test, only analytic validation is needed for commercialization. The FDA established a biomarker qualification program to facilitate the regulatory/industry/academic interface on biomarker development. Additionally, the agency created a regulatory framework that divides biomarkers into exploratory, probable valid, and known valid, each of which can be applied in defined situations during drug development or in the clinic.
There are different tools and analyses that can aid in determining the acceptability to physicians and patients and the impact on the cost-effectiveness of anticancer treatments. The earlier these factors are considered in the drug development program, the more likely they can be optimized so that the potential success of an investigational agent is maximized.
Conclusion
Cancer biomarkers are crucial to discovering and developing novel cancer therapeutics. Devising a biomarker strategy early in the drug development process can help in selecting optimal targets and models for preclinical studies. In turn, this can enhance the probability of success for your preclinical studies while also maximizing the chances for the biomarkers to translate to the clinic. Early biomarker strategies also offer plenty of opportunity to develop a CDx, which will be required for such translation.
Predictive cancer biomarkers are important for making informed risk/benefit assessments that are relevant for individual patients and they can delineate patient populations who would benefit from a targeted therapy or inform dosing or potential safety risks. By linking therapeutics with diagnostics, biomarkers promise to play an important role in advancing personalized medicine.
Cite this Article
Bourré, L., (2020) How to Develop Predictive Cancer Biomarkers - Crown Bioscience. https://blog.crownbio.com/how-to-develop-predictive-cancer-biomarkers
Advancements in oncology are increasingly driven by the ability to extract more detailed and precise information from patient tumor samples. Tradition…
Oncology continues to be a rapidly changing field with scientific discoveries transforming patient treatment and care. As it stands today, advancement…
Cancer research has evolved significantly over the years, driven by the need for more precise and efficient methods to study tumor biology, identify b…