Key Differences between hPBMC and hCD34 Humanized Mouse Models
9:04
SHARE
Learn more about the different human immune cell populations in PBMC and HSC-humanized mouse models, to help select the right model for your studies.
Humanized Mouse Models for Immuno-Oncology Studies
Immunocompetent mouse models are used for many immuno-oncology applications but have limitations regarding specific human immunological mechanisms. These limitations can be partially overcome by using humanized mice.
Humanized mice are generated by inoculation of either human peripheral blood mononuclear cells (PBMC) or hematopoietic stem cells (HSC) into immunodeficient mice. Improvements in immunodeficiency and the introduction of human cytokines such as GM-CSF and IL-3 have expanded the repertoire of human immune cells which develop and engraft in these models. It is important to note that each model has advantages and limitations and experimental criteria are important to determine the proper humanized mouse model selection.
To use humanized mice efficiently, and to be sure that you’re using the right model to answer your specific questions, the presence and potency of the different human immune cell populations in each model need to be fully understood.
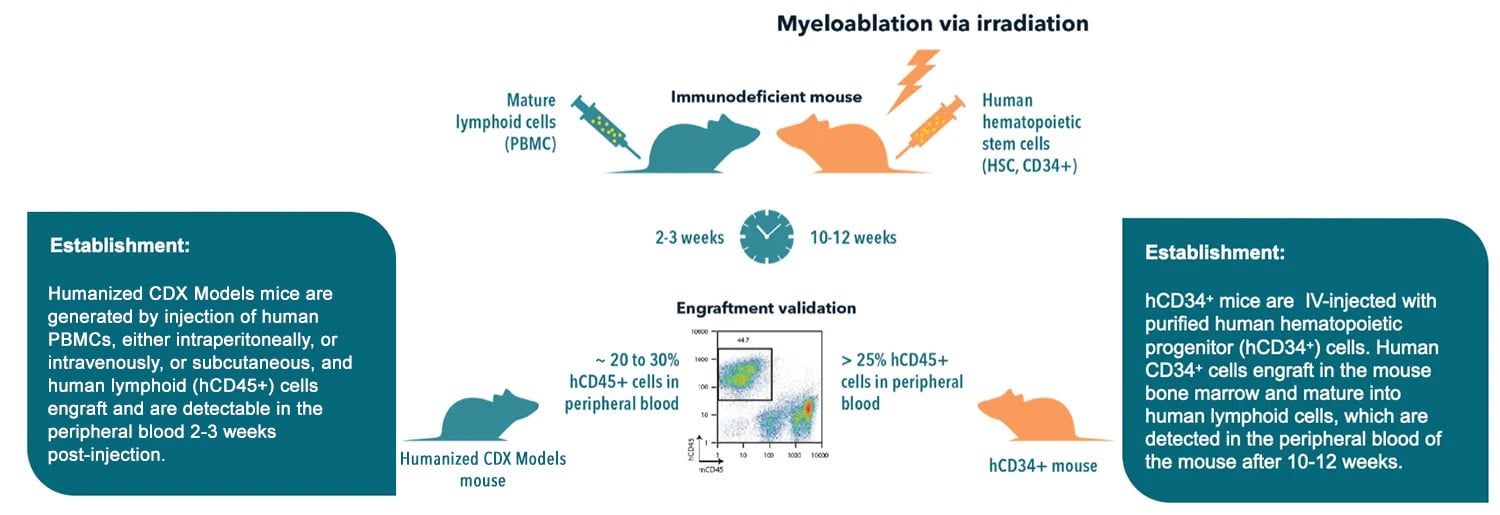
Humanized Mouse Model Generation
Both models support robust human T and B cell engraftment, while hCD34+ mice also show sustainable low level of monocyte and NK cell development. Both models can be engrafted with human tumors for investigations in immuno-oncology (IO).
Humanized Mice Generated with Human PBMCs (Humanized CDX Models)
Humanized mice are generated by injecting PBMCs into immunodeficient mice, such as NSG™/NOG® NCG and BRG mice. PBMC engraftment supports relatively rapid humanization, creating a transient and partially-reconstituted human immune system. The ease of construction and rapid rate of humanization are clear advantages of the hPBMC model.
T Cells
Specifically, a high level of functional and educated T cell populations are present and display and activated and memory phenotype. This model is used to analyze human immune responses in autoimmunity and to gauge cytokine storm induction and irAE.
Uniform T cell activation is observed, dependent upon human PBMC xeno-reactivity with foreign host major histocompatibility (MHC) class I and class II. This leads to rapid GvHD occurrence in a few weeks, limiting length of studies. In order to significantly delay the onset of GvHD and enable longer term studies, knockout mice for murine MHC class I (MHC-KbDb -/-) and/or MHC class II (H2-Ab1-/-) have been successfully used in humanization studies.
Other Hematopoietic Lineages
Engraftment of other important hematopoietic lineages is not supported in this model. This is due to the rapid expansion of T cells, and the lack of cross reactivity of important cytokines for myeloid or lymphoid differentiation, maturation, or activation e.g., IL‐3, IL‐15, GM‐CSF, and macrophage colony stimulating factor (M‐CSF).
For this reason, the majority of myeloid derived cells (i.e., macrophages and dendritic cells [DCs]) are absent and NK cells are present at only a low level.
Also, although the donor humoral repertoire is transferred, PBMC humanized mice show a low level of human B cells with no de novo immune response. This low B cell level is due to a decrease in the proportion of B cells over time, reflecting the strong expansion of T cells. Nevertheless, the absolute number of B cells increases slightly over time and some antibody production has been observed.
Overall, PBMC humanized models can provide significant insight into human tumor immunology and treatment efficacy, targeting T cell function (e.g., agents such as BiTEs, immune checkpoint inhibitors/agonists, CAR-T cell therapy).
Humanized Mice Generated through Hematopoietic Stem Cell Engraftment (HuCD34 Mice)
Alternatively, using human CD34+ hematopoietic stem cells (HSCs) provides a stable, robust model of human immune system engraftment. Humanized mice are generated through inoculating human hematopoietic cells (from cord blood stem cells) into immune deficient mice (e.g., NOG, NSG, BRGSF). For immunotherapies targeting immune cells of myeloid lineages, transgenic immunocompromised mice expressing hGM-CSF and hIL-3 (NOG-EXL and NSG-3GM).
HuCD34 mice cannot support robust adaptive immune responses. Poor B cell response is seen due to incomplete B cell maturation with low levels of IgM and limited class-switching to IgG. To overcome this limitation, hIL-6 knock-in mice have been successfully used. These models show improved T cell engraftment and serum IgG production, with IgG-switched memory B cells displaying a diverse antibody repertoire and high specificity against immunized antigens.
This limitation has also been worked around by expression of human GM-CSF and IL-4 in humanized mice. This improves class-switching, producing significant levels of antigen-specific IgG following immunization.
HLA Molecules
Immunocompromised mice routinely used in CD34+ models do not express HLA molecules on thymic epithelial cells. Due to this limitation T cells are educated and selected on mouse MHC (H2 antigen). This results in T cells unable to recognize antigens in an HLA-restricted manner. To overcome this problem, HLA class I (HLA-A2.1tg or HLA-A2/HHD) and II (HLA-DR1tg or HLA-DR4tg) transgenes were added into NSG mice allowing the development of human T cell repertoires and responses.
Alternatively, BLT (bone marrow, liver, and thymus) mice can also overcome this limitation. The hBLT model is generated by co-xenotransplantation of human fetal liver and thymic tissue under the murine renal capsule, as well as intravenous autologous CD34+ HSC injection. This model shows superior engraftment of hematopoietic lineages with HLA restricted T cells, and it is the only model that leads to the generation of a human mucosal immune system. However, this model is time consuming and challenging due to the surgical procedures involved.
NK Cells and Myeloid Compartment
NK cells are largely absent in HuCD34 mice, and have impaired functionality. With only 65% homology between mouse and human IL-15, supplementation of hIL-15 is essential for development and functionality of human NK cells. Transgenic hIL-15 immunodeficient mice (NSG-hIL15) have been established showing significantly higher levels of human NK cells in comparison to NSG mice. Additionally, higher proportions of human NK cells express granzyme A, B, and perforin compared to NK cells in NSG mice.
The myeloid compartment is also poorly reconstituted in NSG humanized mice. Human myelopoiesis is not efficient in these models, due to the lack of species cross-reactivity of nonhematopoietic cell-derived growth factors including CSF-1, GM-CSF, IL-3, and erythropoietin.
Super immunodeficient murine backgrounds such as NSG-SGM3 and NOG-EXL support enhanced human myeloid cell reconstitution than NSG and NOG mice. HuNSG-SGM3 expresses human SCF, GM-CSF, IL-3, and has higher engraftment of monocytes, macrophages, and DCs compared with the huNSG model. The huNOG-EXL mouse expresses human GM-CSF and IL-3, with higher levels of myeloid cell differentiation following human HSC engraftment compared with huNOG.
It has been published that FLT3-ligand treatment of humanized mice results in higher DCs frequency and functionality. Enhanced myeloid and dendritic cell generation in BRGSF humanized mice show a significant role of myeloid and dendritic cells in CRS development, demonstrating that this is a more relevant and predictive model for the preclinical assessment of CRS and CRS-managing therapies.
In summary, the HuCD34+ model is applicable to assess agents which require multi-lineage immunity. As the human immune system is more fully reconstituted, these models are also useful to investigate more specific mechanistic questions surrounding the stimulation or suppression of the immune response. With the wide therapeutic window, hCD34+ mice are also great for long term studies such as assessing memory response and long-term antitumor effects.
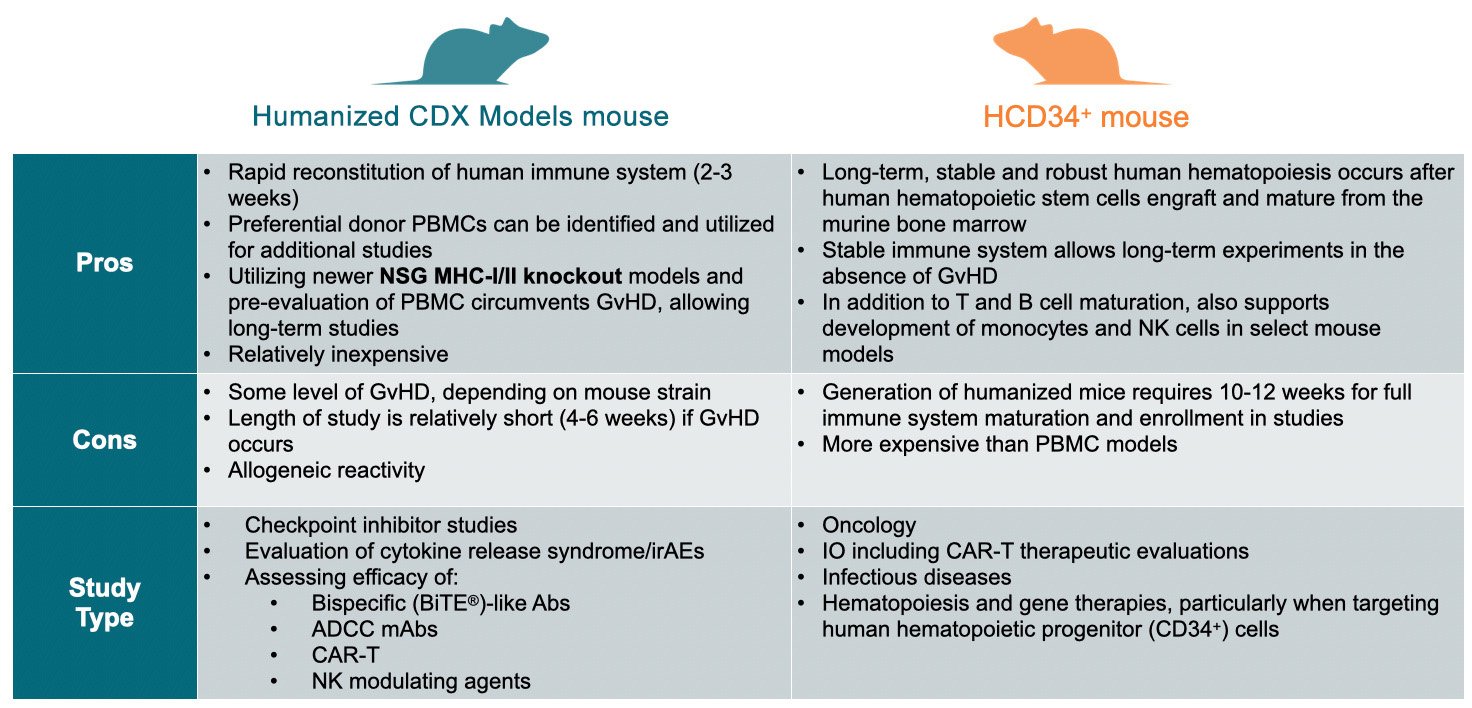
How to Choose the Right Model
Conclusion
Hopefully this guide has provided a brief introduction to the two commonly used humanized mouse model approaches, setting out the advantages and limitations of PBMC and HSC-humanized models, and where you might start in choosing the right model for your studies based on immune cells needed.
Cite this Article
Feuer, G., (2024) Key Differences between hPBMC and hCD34 Humanized Mouse Models - Crown Bioscience. https://blog.crownbio.com/key-differences-between-hpbmc-and-hcd34-humanized-mouse-models
Imagine standing on the brink of a breakthrough in cancer treatment, only to be halted by one daunting barrier: drug resistance. In this episode of Cr…
Oncology drug approvals in H1 2025 In the first half of 2025, the FDA’s Center for Drug Evaluation and Research (CDER) approved a total of 16 novel dr…
Often referred to as “magic bullets” or “biological missiles”, antibody-drug conjugates (ADCs) are one of the most promising advances in targeted canc…