Advanced in vitro technologies to investigate therapeutic impact on the Cancer-Immunity Cycle
Targeting T cells within the Cancer-Immunity Cycle
Analyzing the suppressive tumor microenvironment in in vitro-based assays
What’s next in preclinical cancer immunotherapy research?
In this blog post, we share highlights of our webinar series that explore the CIC, its significance, and how it can be leveraged to facilitate the discovery and development of new cancer immunotherapeutic agents.
What is the Cancer-Immunity Cycle (CIC) and why is it important?
For new cancer immunotherapy agents and treatment regimens to reach their full potential, the interplay between tumor cells, the body’s immune system, and the new cancer immunotherapy agents and treatment regimens must be understood completely. This is why it is important to understand the CIC.
In 2013, Chen and Mellman introduced the CIC as the biological steps required for effective immune-mediated elimination of cancer cells. The steps are as follows:
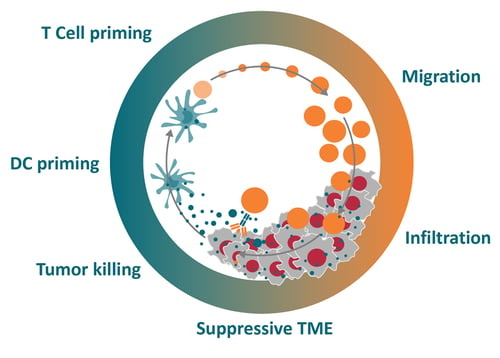
In the first step of the CIC, tumor-specific antigens (neoantigens) are released from dying tumor cells. This is followed by priming of antigen presenting cells (e.g., dendritic cells [DCs]) followed by presentation to naïve T cells in lymph nodes. Upon activation, T cells migrate or are trafficked to the tumor site, where they infiltrate and recognize the tumor as foreign, culminating in the final step where T cells mediate tumor cell killing, further release of antigens and the initiation of another cycle. Figure 1 illustrates the CIC.
Figure 1: The Cancer-Immunity Cycle
How is the CIC regulated?
Under ideal conditions, the CIC operates effectively, leading to tumor cell eradication. The CIC is equipped with a multitude of failsafe mechanisms that enable tight control of the cycle and to prevent autoimmune-mediated damage to normal tissues. Many different stimulatory and inhibitory factors are at play to ensure precise and efficient tumor eradication, including checkpoint proteins such as PD-1 and CTLA4. These factors are essential to controlling T cell response.
Other important CIC regulators are pro-inflammatory cytokines that regulate priming of dendritic cells (e.g., TNF-alpha and IL-1), co-stimulatory factors that influence T cell activation (e.g., CD27 and OX40), and various chemokines that control T cell migration into tumors.
However, in a cancer patient, the CIC can be impaired at any step, such as through ineffective antigen release due to the absence of dying tumor cells or dysfunctional immune checkpoints, which will lead to poor anti-tumor immunity and disease progression.
A major goal of immunotherapy development is to overcome blockades and reactivate the cycle to facilitate tumor recognition and eradication.
Which CIC steps can be targeted with immunotherapies?
Checkpoint proteins, such as CTLA4 and PD-1/PD-L1, are key negative regulators of the T cell anti-tumor immune response. Their blockade with inhibitors releases the “brake” on T cell activity, unleashing a strong immune response against tumor cells. Beyond checkpoint inhibitors, other targeted agents, oncolytic viruses, and traditional therapies (i.e., radiation and chemotherapy) can reignite the CIC by killing tumor cells and promoting antigen release. In addition, therapeutics such as engineered cell therapies (e.g., CAR-T) and bi/tri-specific T cell engagers can modulate and enhance several steps in the CIC that involve T cell activation and migration as well as tumor cell infiltration and eradication. Furthermore, targeting inhibitory cells, such as myeloid suppressors, and other factors within the tumor microenvironment (TME) is thought to be crucial to the success of immunotherapies.
Given the level of complexity of the CIC, preclinical models and tools that allow researchers to dissect each of its steps are needed not only to address specific questions related to anti-tumor immunity but also to identify promising novel immunotherapy targets.
Should I use 2D, 3D, in vivo, or ex vivo models?
A range of preclinical in vitro and in vivo models can be selected for the development of a novel immunotherapy. However, determining which model to use for a specific study is not always easy, since each model has its own benefits and limitations, which should be considered.
Cancer research studies have traditionally relied on 2D systems, but researchers and drug developers are increasingly adopting 3D cell cultures because they recapitulate more faithfully cell to cell interactions, which is known to influence cell signaling, proliferation, viability, and drug response. Organoids, developed using the HUB protocol from adult stem cells in either normal or disease tissue, are highly patient-relevant cultures that faithfully recapitulate the phenotypic, morphologic, and genetic features of the original patient tumor over the long term and after cryopreservation. Organoids have been validated for an increasing number of tumor types. Their unique features include scalability (e.g., for high-throughput screening) and applicability to the development of biobanks and drug screening.
The value of 3D cultures can be further enhanced with immune co-culture assays. These systems can be relatively simple with the addition of a single cell type (e.g., reactive T cells), or more advanced through setups that incorporate multiple cell types (e.g. immune cells and fibroblasts) to recreate key components of the TME. For a more native TME, Crown Bioscience’s 3D Ex Vivo Patient Tissue Platform (EVPT) preserves the intrinsic cell populations found within tissue specimens by placing fresh samples directly into the culture without digestion or pre-culture steps. As a result, EVPT models are ideal for studying the CIC and drug effects, as they contain the full repertoire of cell types found in the TME (i.e., immune cells, stromal cells, and fibroblasts).
Overall, 3D cultures are generally superior to standard 2D cultures for drug discovery in vitro, as they offer higher translational value. Screening for lead candidates can be carried out in low-complexity 3D cultures, and more innovative co-culture systems provide insights beyond viability, such as impact on the TME and other intricate steps in the CIC. The findings from these in vitro experiments can then be used to better inform in-depth studies on preclinical animal models. Prior to embarking on a new study, it is advised that experts be consulted who have deep expertise in selecting the right model for your specific research question(s). At Crown Bioscience, there are a range of preclinical models that have been characterized and information curated in online databases to help identify organoid models, cell lines, and in vivo models.
The rise of high-content imaging (HCI) and analysis (HCA)
HCI and HCA use advanced microscopy and powerful algorithms for drug discovery and validation studies, especially when combined with highly clinically relevant 3D in vitro organoids. Combining these technologies allows you to develop comprehensive cellular profiles that show how compounds affect cellular systems and spatial biology, including the dynamic interactions between cancer cells and immune cells in 3D.
Since HCI provides detailed readouts on individual objects, changes in organoid volume and size, and immune cell proliferation following exposure to T cell engagers, engineered T cells, or checkpoint inhibitors can all be quantified and provide insight into tumor killing. Additional parameters, such as immune cell migration and tumor infiltration, can also be assessed when used with appropriate cell tracker dyes.
HCI has also been instrumental in validating a novel in vitroT cell exhaustion platform. T cell exhaustion occurs when the antigen is not cleared (Step 3 of the CIC), and this weak but chronic activation ultimately leads to an unresponsive state. Since this can impede anti-tumor immunity, assays that recapitulate this process are needed to identify candidates that delay or reverse exhaustion.
HCI can also handle the analysis of more complex cocultures that incorporate additional cellular players beyond T cells and model the TME. For example, cancer-associated fibroblasts (CAFs) play a central role in modulating cancer cell behavior and drug responses. Co-culture systems that model the mesenchymal TME can be generated by mixing tumor organoids with fibroblasts to model tumors consisting of organoids, fibroblasts, and PBMCs. These advanced triple co-cultures benefit from HCI to discriminate between the different cell populations and output accurate measurements of organoid phenotypes and immune cell responses following exposure to immunotherapeutic candidates.
Conclusion
Understanding the Cancer-Immunity Cycle is critical to the development of next-generation immunotherapies. Our new on demand webinar series, The Cancer-Immunity Cycle: Methods, Challenges, and Opportunities provides valuable information on the CIC, including how each of its steps can be studied preclinically to best position your drug candidates for clinical success.
Cite this Article
Kumari, R., (2023) Understanding the Cancer-Immunity Cycle to Improve Cancer Immunotherapy Development - Crown Bioscience. https://blog.crownbio.com/understanding-the-cancer-immunity-cycle-to-improve-cancer-immunotherapy-development
New data from translational research groups, platform developers, and earlystage biotech teams point to a clear trend in 2026: scalable 3D assays and …
Immunooncology (IO) drug development increasingly depends on understanding human specific immune mechanisms. However, these subtle, highly coordinated…
An Interview with Crown Biosciences' SVP of Commercial, Alex Slater Meet Alex Slater, Senior Vice President of Commercial at Crown Bioscience. With a …