Do you ever wonder how tumor organoids and ex vivo microtumors (i.e., patient tumor material) are being used in immuno-oncology (I/O)?
Are you interested in assessing your immunotherapy through tumor organoid co-cultures, with autologous and non-autologous immune cells?
Or maybe you want to explore how ex vivo microtumors can preserve tumor heterogeneity and resident immune cells, removing the need for co-culture systems?
In this blog post, we explore a platform combining 3D models and phenotypic high content imaging (HCI)-based analysis to provide relevant analysis of drug responses that can inform candidate selection and clinical program design.
Challenges in Immunotherapy Drug Development
Preclinical testing of cancer immunotherapies is challenging due to I/O agents needing complex and dynamic interactions between the tumor and immune system to be recapitulated in relevant models.
Current immuno-oncology modelsin vivo are broadly defined as either homograft systems, where the host immune system is intact, or humanized systems where the reconstitution of the human immune system is engrafted in an immunodeficient host. However, there are some limitations to these systems which may obscure efficacy and toxicity associated with an immunotherapeutic. For example:
Species specificity: although homograft models feature a competent immune system they can only be used to evaluate cross-reactive or surrogate agents and thus they only model mouse immunity (not human immunity)
The complexity of humanized systems results in high developmental costs and timelines as well as graft-versus-host disease (GvHD) which limits the experimental window, donor-to-donor variability, and allogeneic response which can complicate data interpretation. In addition, partial or inefficient reconstitution of the immune system can limit the applicability of I/O models to agents targeting non-reconstituted components.
The main challenges in modeling immunotherapy responses in vitro have been:
The limited availability of patient material to test in co-culture systems
The lack of antitumor reactivity of autologous immune cells
Co-culture systems lacking the structural complexity of the tumor microenvironment (TME) to mimic the interaction between immune cells and the tumor.
Tumor organoids are used in co-culture with either autologous or non-autologous immune cells, to provide a patient-relevant in vitro platform for immunotherapy development. Furthermore, as shown later, high content technologies are being used in high-throughput in vitro tumor organoid and immune cell co-culture studies to measure the effects of drugs and combination therapies on physiologically relevant morphological features, such as tumor cell killing, growth arrest, invasion and immune cell proliferation.
The Benefits of Tumor Organoid and Immune Cell Co-Culture
Two major benefits of using in vitro tumor organoids for I/O applications is the enhanced clinical relevance of tumor organoids compared to cancer cell lines and their simplicity in comparison to humanized in vivo systems.
The 3D architecture and spatial arrangement of multiple cell lineages results in the formation of mini-organs that recapitulate the genomic, morphological, and physiological features of the original tumor. The scalability and biobanking of organoids also readily enables the screening of multiple agents against human targets and combinations across different patients and cancer types to better reflect population diversity/heterogeneity and responder/non-responder profiling.
In comparison to in vivo platforms, the in vitro nature of organoid co-culture platforms also makes them highly scalable, which facilitates multiple agent screening and donor/model combinations can be tested at the same time prior to moving forward with more complex in vivo models. Another benefit is that healthy organoids are also available or can be developed simultaneously to evaluate any potential off-target effects on human tissues in parallel, which is not possible with in vivo models.
Tumor Organoid and Autologous Immune Cell Co-Culture
Autologous PBMC and tumor organoid co-cultures are actively in development, and there are some well-recognized challenges associated with this approach, including:
Limited volume of blood from donor cancer patients
Lack of tumor-reactive T cells among PBMC from most donor patients
Limited scalability for drug development applications
Tumor Organoid and Non-Autologous Immune Cell Co-Cultures
A more feasible approach for immuno-oncology drug development is the use of organoid and non-autologous immune cell co-cultures which overcome some of the challenges discussed above. Non-autologous immune cells are much more readily available from healthy donors. Here, rather than using matched organoid and immune cells, the organoid or immune cells are selected based on different criteria.
Organoids are selected based on the gene or protein expression profile of a target of interest or mutational burden using Crown Bioscience’s Organoid Models Database
Multiple non-autologous immune cells donors can be selected, or different immune cells isolated, or HLA-matched
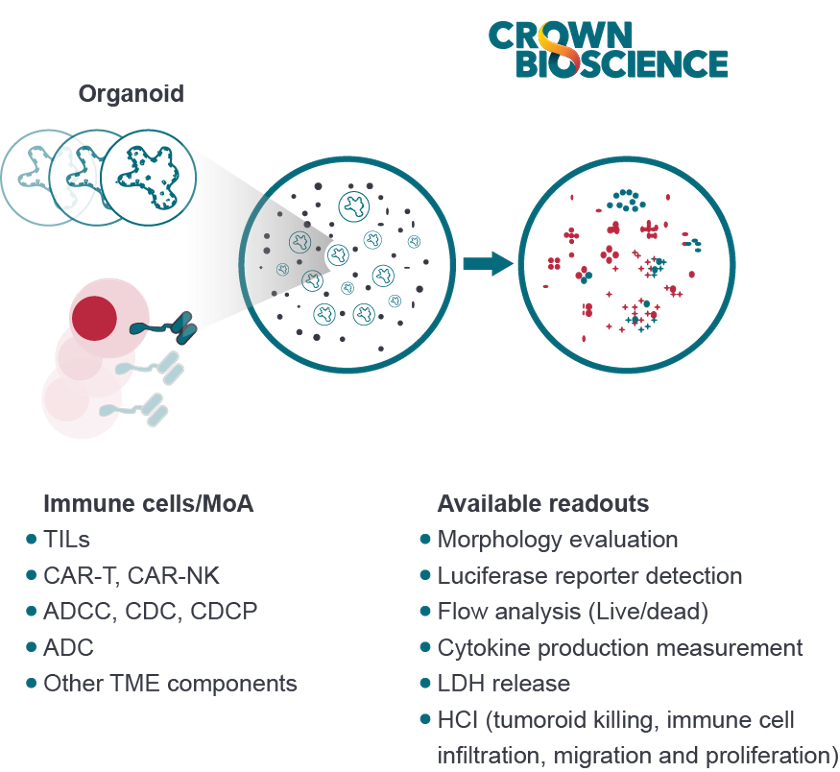
Tumor organoid and non-autologous immune cell co-culture platforms are used to assess:
Tumor organoid killing by allogeneic T cells to evaluate the potency of immunotherapy agents
Tumor organoid killing and tumor reactivity of CAR-T and TCR T cells
Tumor organoid killing by ADCC (NK) and ADCP (macrophages)
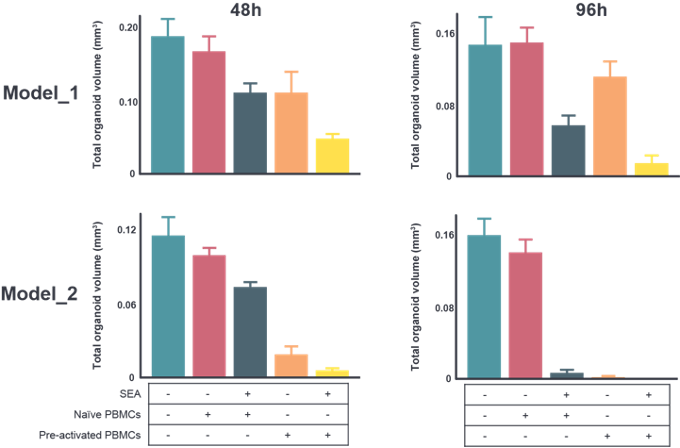
In the example below, two different colorectal cancer (CRC) organoid models were co-cultured with differentially pre-treated HLA-matched PBMCs (naïve, naïve with superantigen [SEA], pre-activated with SEA, pre-activated and re-activated with SEA).
Immune cells were pre-labelled before adding them to the co-culture and HCI was performed to assess immune cell-mediated organoid killing over time, based on organoid tumor volume at different time points. Differential killing was observed depending on the activation status of immune cells and immunogenicity of each organoid model.
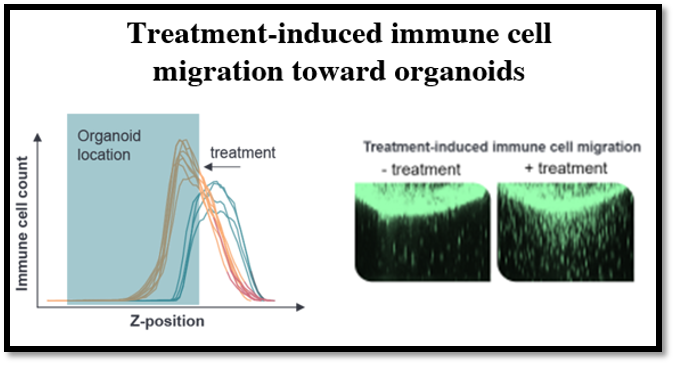
Immune cell migration can also be tracked by following stained immune cells that are added to the top of the hydrogel layer containing tumor organoids. Using HCI and image analysis, the number of immune cells is scored in different z-positions within the hydrogel and their distance towards the organoids can be analyzed.
Challenges of Tumor Organoid and Non-Autologous Immune Cell Co-Culture
There are still some challenges associated with co-culturing organoids with non-autologous immune cells. These co-cultures cannot be used to test tumor antigen specificity. Organoid co-cultures with non-autologous T cells test the allogenic T cell response/killing of tumor organoids and measures the potency of immune checkpoint inhibitors. However, in the clinical setting, checkpoint inhibitors are aimed at improving T cell response to specific tumor antigens, instead of eliciting allogenic T cell responses. Further development of the organoid and non-autologous immune cell platform should allow the testing of tumor antigen specific T cell reactivity.
Tumor Organoid Killing with CAR-T Cell Co-Cultures
Tumor organoid killing by CAR-T cells has been investigated using several technologies, including ELISA, luminescence-based analysis of engineered organoids, morphology analysis, and FACS analysis. Three studies are summarized below to highlight how tumor organoid and CAR-T cell co-cultures can be used to investigate CAR-T cell efficacy.
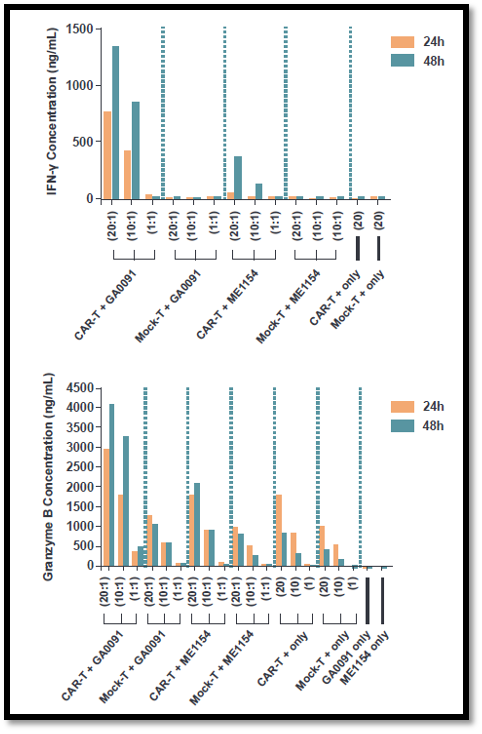
In a study conducted by scientists at Crown Bioscience, researchers compared the effects of EpCAM CAR-T cells on two tumor organoid types: gastric cancer organoid GA0091 (EpCAM+) and melanoma organoid ME1154 (EpCAM-).
The EpCAM CAR-T cells were cocultured with the two organoid types at different effector:target (E:T) ratios, and the co-culture supernatants were analyzed by ELISA for cytokine production after 24 or 48 hours. ELISA analysis demonstrated that EpCAM CAR-T cells caused a significant rise in the levels of IFN-γ and Granzyme B in the supernatant of EpCAM+ GA0091co-cultures, suggesting effective CAR-T cell reactivity against EpCAM+ GA0091 gastric tumor organoids (see graphs below).
In a second study, liver tumor organoids (PDXO LI6677) were engineered to express luciferase and human CD19, and subsequently co-cultured with CD19 CAR-T cells for 2 days.
Luminescence-based analysis was then used to track organoid growth/death. The investigators reported that luciferase activity was successfully used to track killing of the tumor organoids (see graph below).
In a third study, lung tumor organoids (LU6438 B7H3+) were co-cultured with human B7H3 CAR-T cells at a 2:1 ratio for 3 days. B7H3+ organoid killing with B7H3 CAR-T cells was tracked using morphological changes assessed by HCI, and marker analysis by FACS. While killing did not occur with non-antigen-specific CAR-T cells, marker analysis with FACS at day 4 confirmed the killing effect.
Overall, tumor organoid co-cultures are in vitro models that are more clinically relevant compared to cancer cell lines, and a higher scalability than in vivo models. Tumor organoid models that express specific tumor antigens can be selected using our Organoid Models Database and as shown above, several different assays can be used to evaluate CAR-T cell reactivity to tumor organoids.
Engineering Tumor Organoids to Develop Unique New Immunotherapy Models
Another distinct advantage of tumor organoids for I/O applications, relative to in vivo models, is that they can be engineered to establish new immunotherapy models, such as by expressing specific CAR-T targets of choice. These models can also be modified to express luciferase or fluorescence reporters which allow the detection of tumor organoid killing via imaging.
3D Ex Vivo Microtumors: A Case Study to Highlight the Power of HCI in I/O
As described previously, the term “High Content” largely refers to the fact that many morphological parameters/features (which are measured using fluorescent dyes) of individual cells can be simultaneously evaluated in an automated fashion, such as cell cycle status, cellular and nuclear morphology, cell viability, receptor internalization, and protein aggregation.
This technology is now being applied to 3D ex vivo microtumors (i.e., patient tumor material) that preserve the native tumor architecture, and TME that contains components that express important drug targets, which play a critical role in both tumor progression and modulation of the response to drugs. This approach can therefore improve response predictability to I/O candidates.
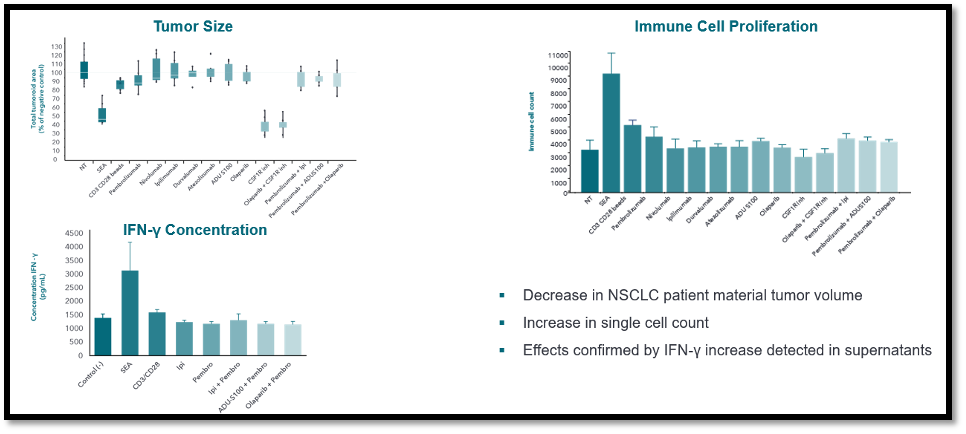
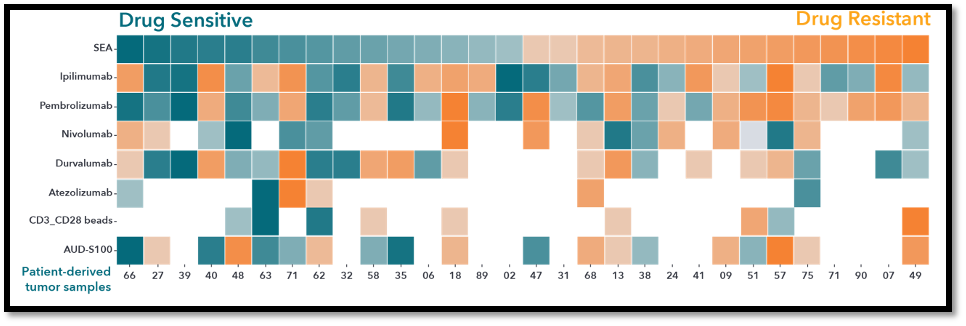
Overall, the platform successfully demonstrated the utility of ex vivo drug testing protocols for determining drug sensitivity using fresh patient tumor tissue with preserved TME components in combination with advanced 3D HCI-analysis. The first image below shows a decrease in NSCLC patient material tumor volume, elevated single cell counts, and an increase in IFN-γ increase in the supernatants, while the second shows a heatmap of drug sensitivity across different drugs and ex vivo microtumors.
Conclusion
Tumor organoids have certainly started to bridge the gap between tissue culture systems and patients in the clinic. Using tumor organoids for immuno-oncology applications offers researchers an attractive additional preclinical option for modeling the complexities of tumors in vitro for scalable I/O drug development including drug combinations on different cancer types.
While the use of tumor organoids allows the reconstitution of the TME by incorporating different cellular players in one co-culture, the 3D ex vivo tumor cultures contain an intact TME from the patient.
Combining these culture systems with HCI-based analysis allows researchers to obtain highly detailed quantification of tumor sensitivity to I/O drugs.
These patient-relevant models can significantly improve the preclinical evaluation of I/O drugs, and also to potentially improve the success rate of clinical trials.
Cite this Article
Kumari, R., (2022) Using Tumor Organoids and 3D Ex Vivo Microtumors for Immuno-Oncology Applications - Crown Bioscience. https://blog.crownbio.com/using-tumor-organoids-and-3d-ex-vivo-microtumors-for-immuno-oncology-applications
New data from translational research groups, platform developers, and earlystage biotech teams point to a clear trend in 2026: scalable 3D assays and …
Immunooncology (IO) drug development increasingly depends on understanding human specific immune mechanisms. However, these subtle, highly coordinated…
An Interview with Crown Biosciences' SVP of Commercial, Alex Slater Meet Alex Slater, Senior Vice President of Commercial at Crown Bioscience. With a …