One key aspect of T cell therapy is to identify tumor antigen targets which can be recognized by T cell receptors (TCR) on cytotoxic T lymphocytes and induce malignant cell death. Selecting specific antigens within a patient’s tumor cell repertoire allows for highly personalized cancer therapy.
In general, the best type of tumor antigen target exhibits several features:
High tumor specificity - expressed in tumors, but with either no or very low expression in normal tissue.
Tumor addiction - related to oncogenesis.
High immunogenicity - able to induce T cell response.
There are two major classes of tumor antigen which can be exploited for T cell therapies - public shared antigens and private antigens (also known as neoantigens).
Public Shared Antigens
Public shared antigens are common to multiple patients and are themselves split into two further categories:
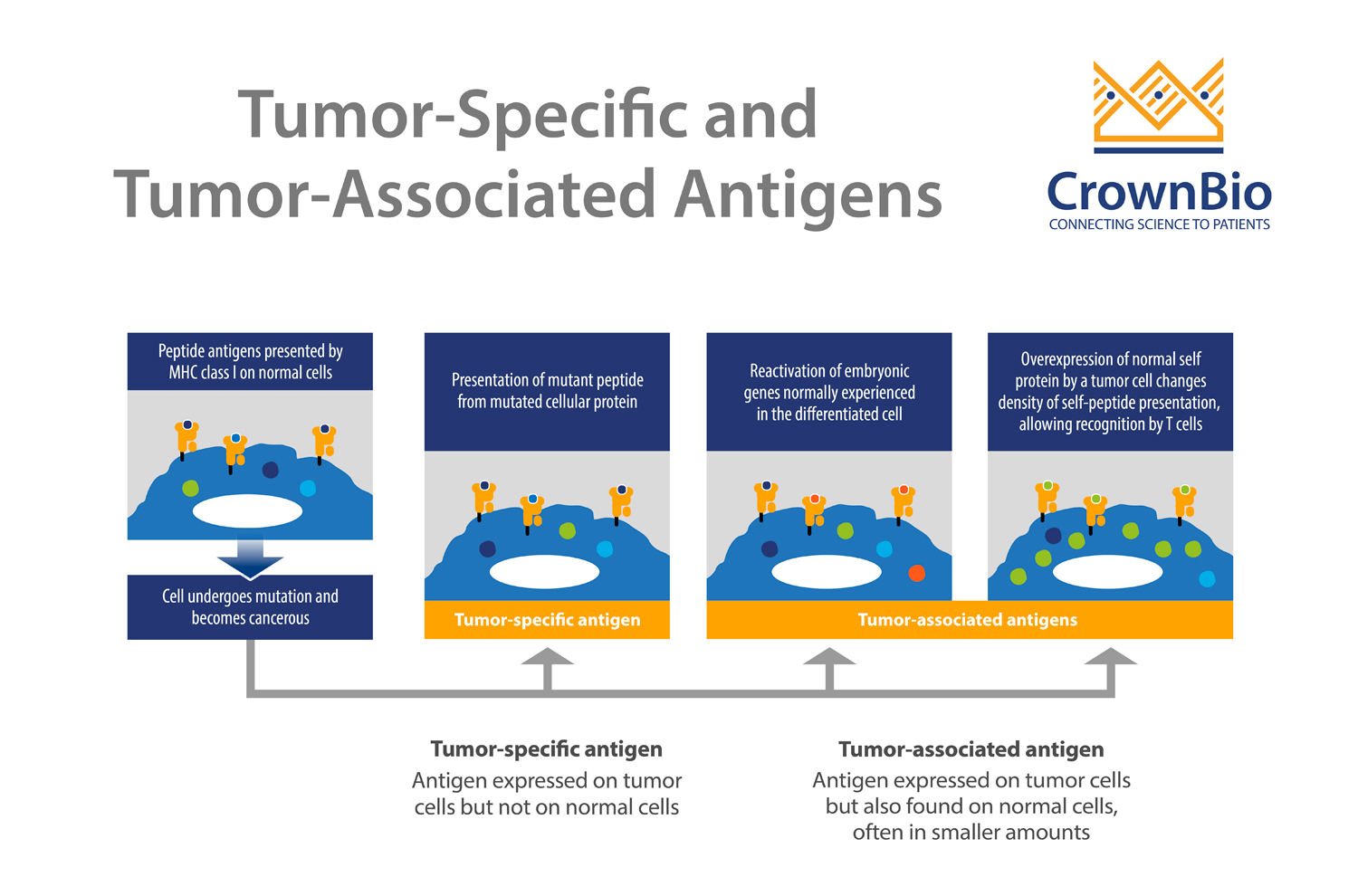
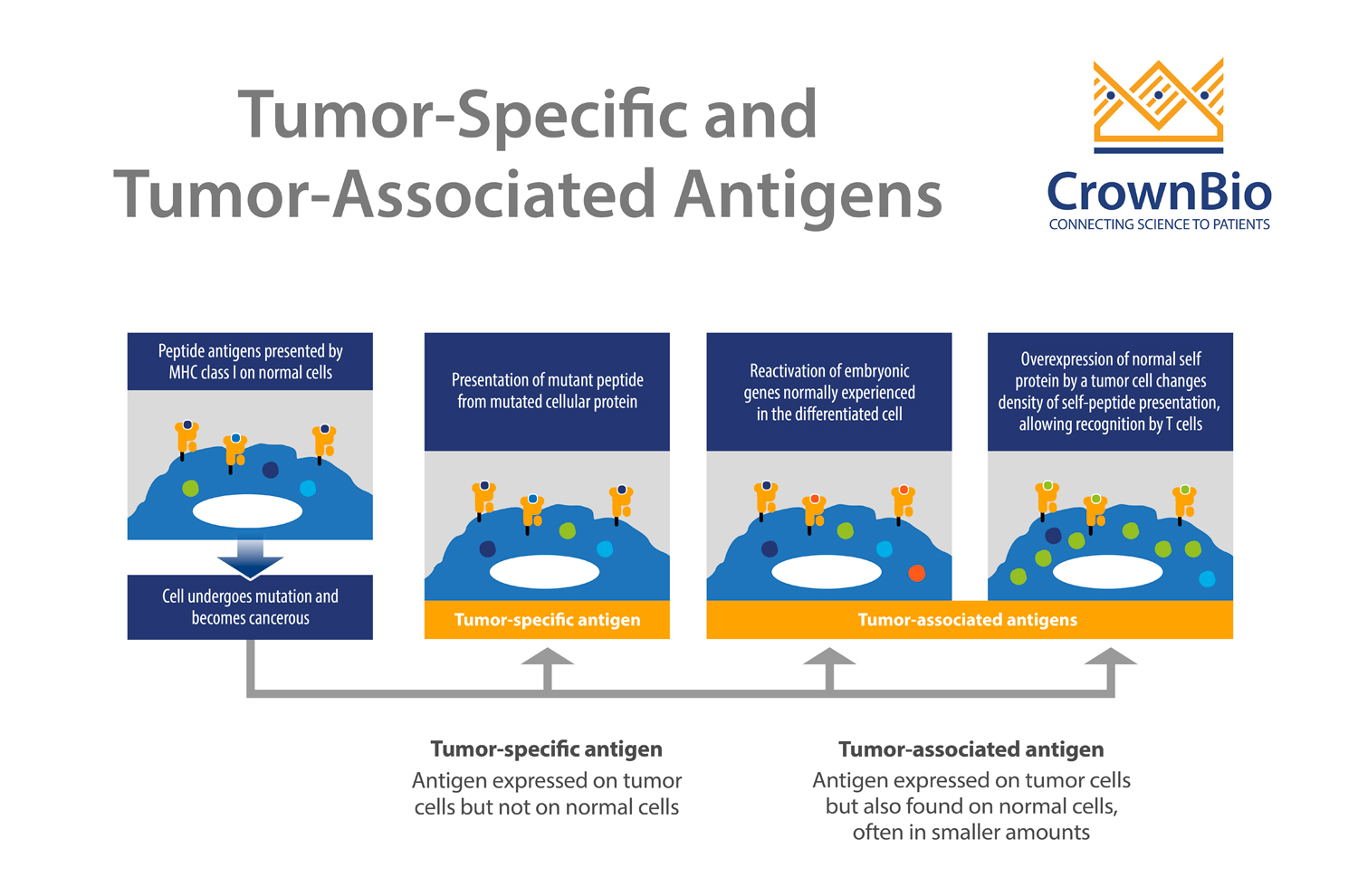
Tumor-specific antigens (TSA), which are found on cancer cells but not on healthy cells.
Tumor-associated antigens (TAA), which have elevated levels within tumor cells, but can be expressed by healthy cells at lower levels.
Public antigens have shown promising clinical success and can be developed as an “off-the-shelf” T cell therapy. However, this can result in autoimmune disease development due to off-target effects.
Public Antigen Targets in Preclinical Trials
Multiple public shared antigens have been assessed preclinically. This includes several antigens which have been identified through gene expression profiling as specifically highly-expressed in tumor samples.
One pair of identified antigens are melanoma-associated antigens recognized by T cells (MART)-1 and glycoprotein 100 (gp100), which are widely studied targets in treating metastatic melanoma. They are melanocytic differentiation antigens overexpressed by melanoma cells in the skin, eye, and ears.
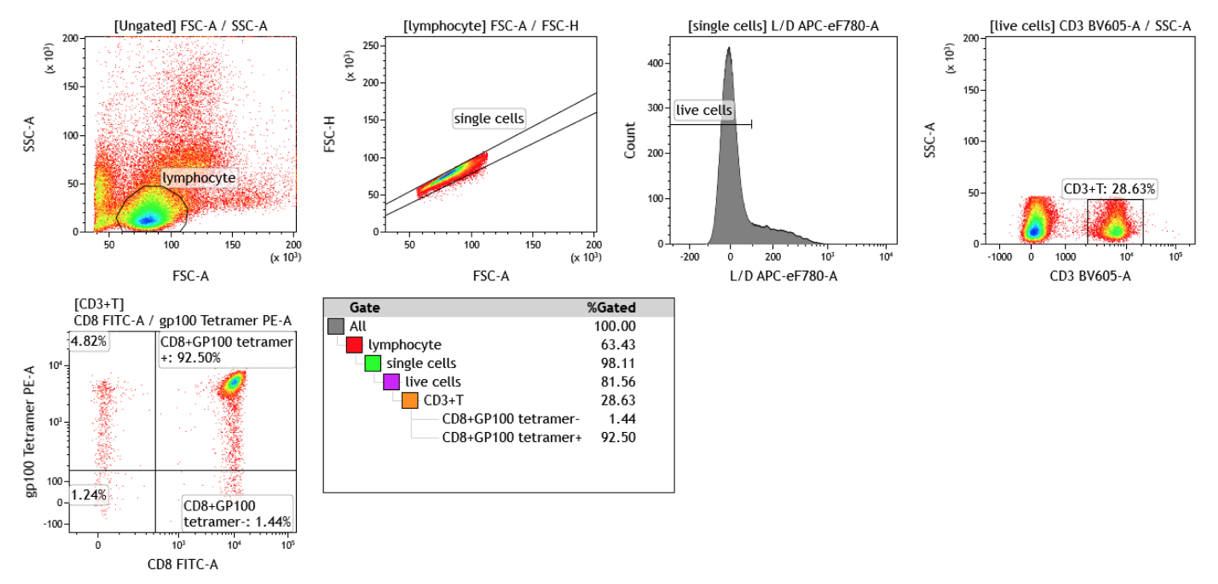
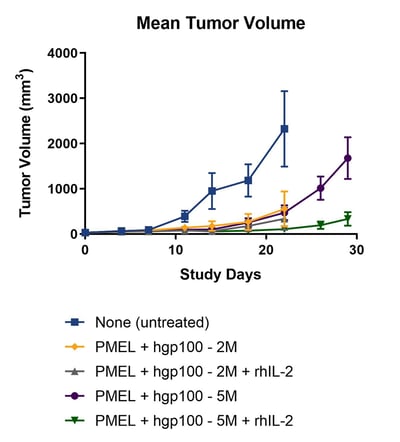
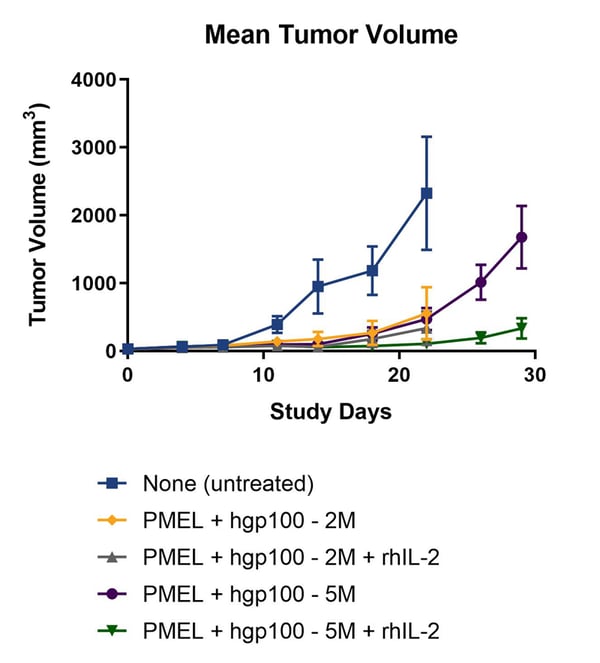
Preclinical evaluation has included using a mouse model platform to mimic ACT of antigen-specific T cells. This platform uses a transgenic mouse model carrying a TCR transgene specific for Pmel-17, the mouse homologue of human gp100.
Adoptive transfer of a gp100 peptide activated Pmel-17 specific T cells in lymphodepleted recipient C57/BL6 animals. This rapidly caused regression of large cutaneous murine B16-F10 melanoma.
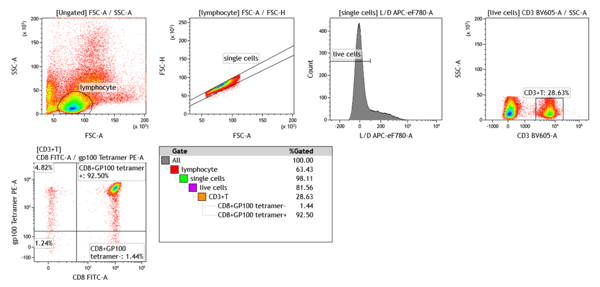
gp100 tetramer peptide induces melanoma regression in Pmel-17 transgenic mice
Public Antigen Targets in Clinical Trials
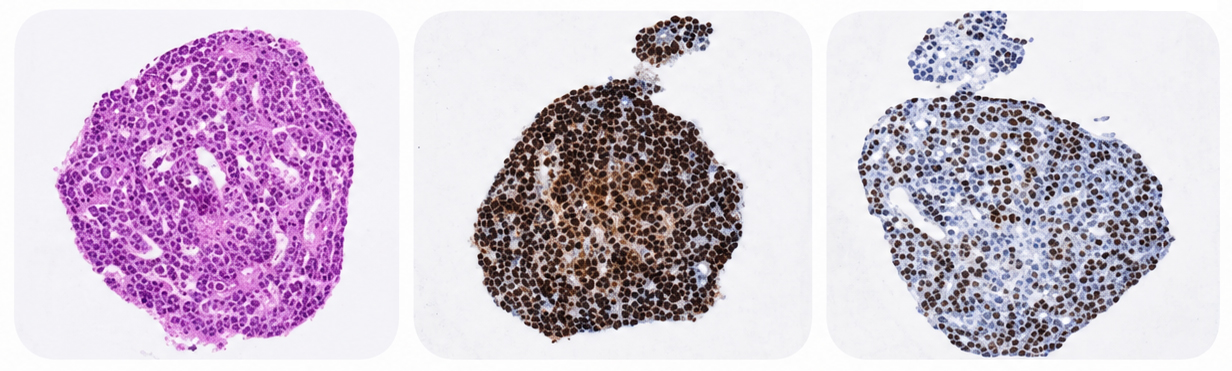
Targeting these antigens has carried on into Phase I and II clinical studies. MART-1 and gp100 TCR-engineered CTL mediated increased inflammatory cytokine expression and tumor regression in metastatic melanoma. pHMC tetramers coupled with a fluorochrome by flow cytometry techniques were able to identify accumulation of these antigen specific T cells at tumor sites
Melanoma-associated antigen (MAGE) T cells (MAGE-A10, MAGE-A4) are currently under clinical evaluation for multiple malignancies including urinary bladder cancer, head and neck cancer, melanoma, and non-small cell lung cancer (NSCLC), led by Adaptimmune.
Clinical trials of New York Esophageal Squamous Cell Carcinoma (NY-ESO)-1 targeting T cells against bone sarcoma, soft tissue sarcoma, advanced non-small cell lung cancer, and synovial sarcoma are also ongoing. In a pilot trial, simultaneous delivery of NY-ESO-1-specific T cells with NY-ESO-1 peptide pulsed dendritic cells into patients with advanced carcinoma or melanoma resulted in regression in 50% of subjects.
Private Antigens
Neoantigens are also known as private antigens and are specific to a single patient. They are non-self peptides derived from nonsynonymous burden somatic mutations unique to cancer cells. The advantage of neoantigens over public antigens is that they have not gone through thymus selection and therefore the host immune system identifies them as “non-self”.
Due to the absence of these antigens in normal cells, neoantigens are potentially more immunogenic than shared antigens, and unlikely to contribute to autoimmunity. However, only 1% of tumor mutations result in true neoantigens.
Targeting private antigens may reduce the chance of off-target effects, but this personalized treatment approach is intrinsically much more expensive and time-consuming due to the time and effort needed to identify neoantigens.
Identifying Private Antigens
Next generation sequencing of tumors and matched normal tissue samples can be used to identify neoantigen candidates for personalized treatment. Peptide exchange MHC tetramer platforms are available to screen and validate peptides and neo-epitopes. This method identifies the peptides binding to MHC class I pockets and determines the strength of their binding to the cleft of MHC-I.
ACT Targeting Neoantigens in the Clinic
Clinical trials have been performed targeting private antigens. Zacharakis and colleagues demonstrated adoptive transfer of tumor infiltrating lymphocytes against four different neoantigens, in combination with IL-2 and immune checkpoint inhibitors. This mediated a complete and durable regression of ER+/HER2-negative metastatic breast cancer.
In August 2018 the National Cancer Institute launched a Phase II clinical trial on autologous ACT of TCR against neoantigens in patients with metastatic cancers, including glioblastoma, non-small cell lung, ovarian, breast and gastrointestinal/genitourinary cancers.
Some of the neoantigens seemed to be shared among a subpopulation of cancer patients, and ongoing studies are underway to identify other shared neoantigens common to larger patient populations. For example, for HLA-B*15:03, KQMNDARHG, and for HLA-A*30:01 and HLA-B*15:17, LSKITEQEK and STRDPLSKI, were identified most often in breast carcinoma patients.
Summary
Persistent activation, expansion, and enrichment of antigen-specific T cells has shown promising therapeutic tumor-killing effects. While public antigen targets are readily identified and can be offered as an off-the-shelf product, safety and efficacy issues pose major concerns.
Neoantigen targets are likely safer and effective compared to public antigens, but are disadvantaged by the time and cost in identifying neoantigens in a patient for personalized therapy.
Cite this Article
E, A., (2019) Tumor Antigen Targets for Personalized Adoptive T Cell Therapies - Crown Bioscience. https://blog.crownbio.com/tumor-antigens-t-cell-therapy
New data from translational research groups, platform developers, and earlystage biotech teams point to a clear trend in 2026: scalable 3D assays and …
Immunooncology (IO) drug development increasingly depends on understanding human specific immune mechanisms. However, these subtle, highly coordinated…
An Interview with Crown Biosciences' SVP of Commercial, Alex Slater Meet Alex Slater, Senior Vice President of Commercial at Crown Bioscience. With a …