Explore how patient-derived tumor organoids are used in the clinic to develop novel precision medicine approaches for guiding and informing treatment options.
Patient-derived tumor organoids are a transformative preclinical oncology model system. 3D organoids are derived directly from patient tumor tissue, using culture conditions specifically designed to preserve the cancer stem cell (CSC) component of the originating tumor. As a result, organoids faithfully recapitulate originating tumor complexity, due to the CSCs ability for self-renewal and differentiation into the multiple cell types found in the original tumor.
Hubrecht Organoid Technology (HUB) protocols, based on methods first developed in the Clevers lab, are pioneering protocols for developing patient-derived tumor organoids. These methods employ a cocktail of growth factors, without a feeder cell layer to generate robust tumor organoids, closely recapitulating several properties of the original tumor.
Tumor Organoids Recapitulate the Original Tumor Tissue
Patient-derived tumor organoids contain both CSCs and their downstream, more-differentiated progeny. Tumor organoids also share genomic characteristics with their primary tumor. For example, pancreatic tumor organoids have been shown to maintain oncogenic alterations (e.g. KRAS, TP53, SMAD, CDKN2A, amplified MYC) and loss of tumor suppressors TGFBR2 and DCC.
Tumor organoids also exhibit morphologic structures reminiscent of primary tumor histology, e.g. pancreatic, colon, breast, prostate, lung, liver, etc. This can include developing an invasive phenotype typical of metastatic tumors. Gene and protein expression are also similar to those seen in corresponding primary tumor cell subtypes.
Tumor Organoids Enable Precision Medicine Approaches
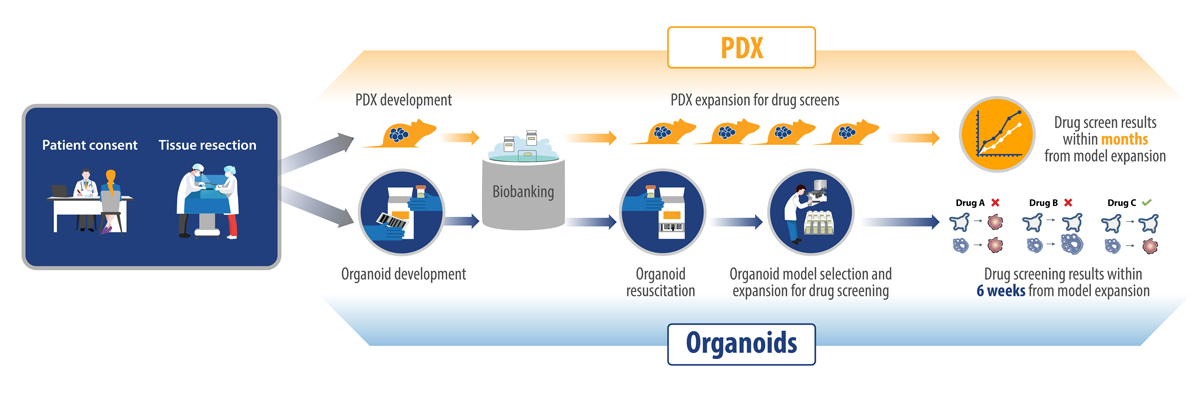
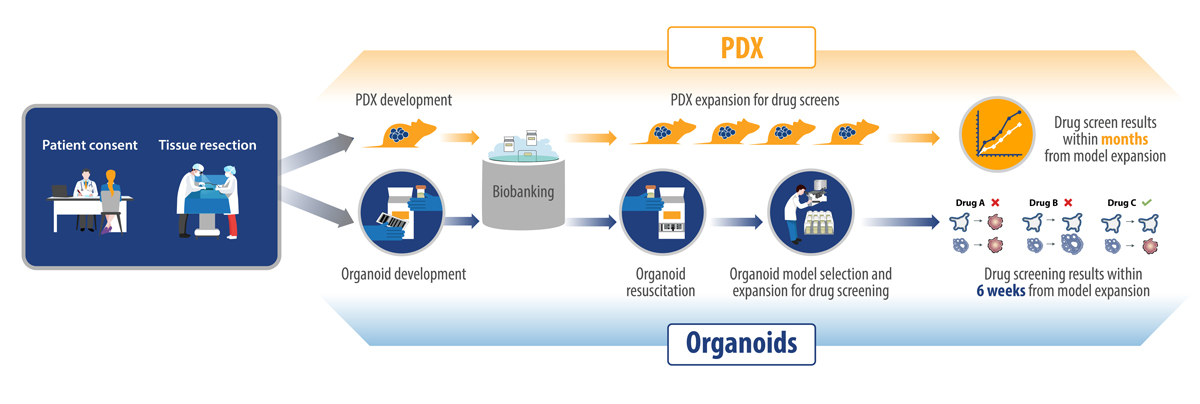
Precision medicine is being increasingly used in oncology to help select the best therapy for a specific patient. While patient-derived xenografts (PDX) showed some promise for precision medicine, they take time to develop, can be costly, and are not easily scaled.
Since tumor organoids are also patient-derived models, they are similar to PDX in that they preserve original tumor characteristics and patient relevance, as well as being predictive of patient treatment response. The added benefits of tumor organoids over PDX for enabling precision medicine approaches is that they are faster to develop and more easily scalable.
Tumor organoids allow the testing of a wide variety of possible therapies, many of which might not be standard of care for the indication in question. These results can potentially be combined with other tests, like genomic screens, to determine mechanisms of resistance or alternative therapeutic options.
A typical workflow for these types of studies is:
Establish patient-derived tumor organoids using biopsies obtained from cancer patients, which may be treatment naïve or have failed previous therapies
Establish and expand the tumor organoid cultures
Perform in vitro screens using the tumor organoids and a variety of anticancer treatments (alone or in combination), such as chemotherapies, radiation, etc.
Some technical and translational considerations need to be kept in mind when comparing ex vivo organoid and patient response. Firstly, not all tumors will develop into organoids - the take rate, for example, is lower for low grade tumors.
Additionally, organoid culture conditions are optimized for epithelial, therefore the tumor microenvironment contribution to tumor therapy response can’t be evaluated unless autologous immune cells and stroma are also available. Autologous organoid and immune cell co-cultures are currently being researched, but it’s early days. Protocols still need to be optimized for multiple tumor and immune cell types before they can be applied to evaluating patient response.
Clinical Trials Using Tumor Organoids
Clinical trials using tumor organoids as a readout fall into two main categories:
Guiding patient treatment options. In these trials tumor organoids are established from cancer patients, and drug sensitivity data are used to guide treatment options for these patients in real time. Treatment options are devised based on the tumor organoid drug sensitivity data.
For example, an upcoming innovative clinical trial (the ORGANOTREAT-01 trial run by the Gustave Roussy/INSERM in Paris) proposes to use tumor organoids to generate a personalized chemogram for patients, and identify unexpected therapeutic options for them. Biopsies will be taken from patients with advanced colorectal cancer and other digestive cancers as they are finishing their last line of treatment.
The resulting patient-derived tumor organoids will then be used to test a panel of 26 treatments to evaluate antitumor activity within 6 weeks, and suggest additional or alternative therapies as quickly as possible. A secondary objective is to evaluate the proportion of patients treated according to the chemograms, and the efficacy of the different regimens.
Informing on treatment options for subsequent patients with shared tumor characteristics. In these trials, patients and their derived tumor organoids are treated with the same drug regimens. Clinical outcomes and tumor organoid drug sensitivity data are then compared. The main goal of these studies is to use the data downstream, to inform treatment options for later patients with shared tumor characteristics.
A recent co-clinical study developed metastatic colorectal cancer organoids to evaluate the drug response in the organoids compared to the patient they were derived from. Across targeted agents and chemotherapy the organoids had a 100% negative predictive value and 89% positive predictive power, demonstrating the clinical relevance of tumor organoids.
Conclusion
Patient-derived tumor organoids are positioned to transform cancer precision medicine due to their faithful recapitulation of parental tumor complexity, and their amenability for rapid, multi agent testing. These ongoing clinical trials will validate the applicability of tumor organoids for precision medicine, allowing guidance of patient treatment.
Cite this Article
Kumari, R., (2020) The Role of Patient-Derived Tumor Organoids in Precision Medicine - Crown Bioscience. https://blog.crownbio.com/patient-derived-tumor-organoids-in-precision-medicine
Imagine standing on the brink of a breakthrough in cancer treatment, only to be halted by one daunting barrier: drug resistance. In this episode of Cr…
Oncology drug approvals in H1 2025 In the first half of 2025, the FDA’s Center for Drug Evaluation and Research (CDER) approved a total of 16 novel dr…
Often referred to as “magic bullets” or “biological missiles”, antibody-drug conjugates (ADCs) are one of the most promising advances in targeted canc…