Although radiotherapy (also called radiation therapy) is an important aspect of cancer treatment, it has limitations, including its potential for damaging healthy tissues, induction of radiotherapy resistance, requiring well-oxygenated tumors, and potentially increasing the risk for generating metastases. There remains an unmet need for ways to enhance radiotherapy.
In this blog post, we explore the value of using clinically predictive patient-derived tumor organoids (PDOs) to discover the radiosensitizing effects of existing standard-of-care (SoC) drugs or novel compounds.
Benefits and Challenges of Radiotherapy in Cancer Treatment
The direct and indirect effects of radiotherapy cause extensive DNA and cellular damage. For instance, the indirect effects of radiotherapy occur mostly due to the generation of high levels of reactive oxygen species (ROS), which can lead to the formation of highly cytotoxic DSBs and other cellular damage. These types of damage can cause cell death or permanent growth arrest. Overall, many factors have been shown to affect tumors’ response to radiotherapy, including:
Cancer cell genetics/epigenetics
The tumor microenvironment (TME)
Cancer cell metabolism.
While radiotherapy has established benefits in the treatment of cancer, there are also several well-known challenges associated with the use of this therapy. As noted earlier, radiotherapy can cause substantial damage to healthy tissue, and radiotherapy has also been shown to mobilize tumor cells into the circulatory system (especially if the treatment does not kill most cancer cells present), possibly leading to a higher risk of metastasis. Radioresistance is another challenge; this occurs when cancer cells survive and proliferate despite the substantial genomic damage brought on by radiotherapy.
While the exact mechanism(s) of radioresistance remains under investigation, it is believed to involve alterations that change the expression of key genes, such as those involved in the DNA damage response (DDR) pathway, chromatin remodeling, cellular metabolism, and changes within the TME.
The Value of Radiosensitizers
Attempts at improving radiotherapy have mostly focused on enhancing the delivery of high-energy photons to the tumor (e.g., improving the precision and accuracy of delivery) and the use of compounds known as radiosensitizers, which are defined as 'any substance that makes tumor cells easier to kill with radiation therapy.’
Many SoC anti-cancer drugs are radiosensitizers, including gemcitabine, interferon-alpha, ErbB inhibitors, doxorubicin, docetaxel, cisplatin, methotrexate, 5-FU, and bleomycin (among others).
At a high level, radiosensitizers are grouped into three categories based on their structures— small molecules, macromolecules, and nanomaterials. Although each type of radiosensitizer has its own set of advantages and disadvantages, their general mechanisms fall into the following categories:
Inflicting additional direct DNA damage (beyond that of radiotherapy alone)
Inhibiting DNA repair mechanisms
Enhancing cell functions that improve cytotoxicity
Altering the expression of radiation resistance and/or radiation-sensitive genes.
The efficacy of radiosensitizers largely depends on the type and dose of the drug, the dose of radiation, and the time interval between the radiotherapy and the radiosensitizer. Despite the radiosensitizing properties of SoC drugs and progress in developing novel radiosensitizers, there is an immediate need to identify more effective radiosensitizers.
As described previously, 3D in vitro organoids are microscopic self-organizing structures grown from adult stem cells (ASCs), and they recapitulate the key structural and functional properties of the original source.
Optimized Hubrecht Organoid Technology (HUB) protocols have been established to develop models from both normal and diseased tissues, including tumor tissue. Patient-derived tumor organoid models can be produced either directly from patient tissue, known as PDOs, or from patient tissue that has been cultured in mice as patient-derived xenografts (PDXs), which are subsequently used to generate patient-derived xenograft organoids (PDXOs); both of which represent alternatives to working with primary patient cells.
Such 3D in vitro tumor models faithfully recapitulate the genomic, morphological, and pathophysiological characteristics of the original patient tumor and are more easily scalable than in vivo models. That is, they are amenable to HTS approaches, and they are genetically and phenotypically stable even after long-term culturing and cryopreservation.
PDOs are important models being used to discover novel sensitivities to radiotherapy alone and in combination with potential radiosensitizers, including SoC anticancer therapies. For instance, one study exposed ten PDO models to a range of radiotherapy plus or minus a toxic dose of cisplatin or cetuximab. The combination of chemotherapy and radiotherapy resulted in increased cell death compared with single-agent treatment, and sensitivity to radiotherapy was increased in the presence of cisplatin in six of ten tested lines and in four of ten combined with cetuximab.
Furthermore, the radiosensitivity of the organoids was compared to the clinical response. For six out of seven patients, the organoid response toward radiation was similar to the clinical outcome of the patient.
Overall, PDOs are increasingly recognized as highly clinically predictive models used to develop in-depth data rapidly. These data can help develop novel approaches to radiotherapy that can lead to better cancer treatment options and outcomes for patients.
Novel PDO Radiosensitizer Screening Platform
As noted, 3D tumor organoids are amenable to HTS approaches, which can help discover the radiosensitizing effects of existing drugs or novel compounds. This approach can also be used to assess the specificity of the radiosensitizing effect by comparing organoids derived from tumor tissue with those derived from corresponding normal tissue.
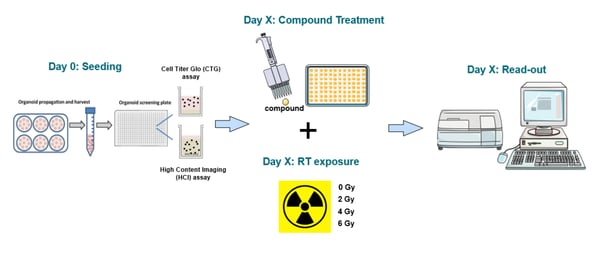
Using a validated platform that is flexible, robust, and reproducible, means that clear differences in radiosensitivity across PDO models can be reliably demonstrated. An example experimental workflow is shown in Figure 1. After propagating, harvesting, and plating organoids, they are exposed to the desired compounds in the presence or absence of different levels of radiation.
Readouts are then obtained using standard biochemical viability assays, such as CellTiter-Glo (CTG) or high-content imaging (HCI), which allows a vast variety of readouts in 3D organoids, including tumor cell killing, target expression, antibody binding, and many morphological parameters. HCI can even discriminate between compounds that induce cell cycle arrest, apoptosis, and necrosis.
Figure 1: Example experimental HTS workflow for identifying radiosensitizers using PDOs.
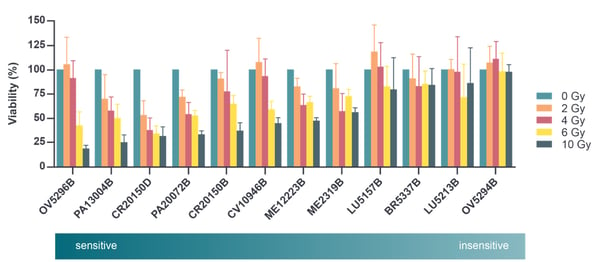
Below are the results of an experimental study that investigated the sensitivity of 12 PDO models to radiation. PDOs were exposed to radiation levels ranging from 0 to 10 Gy. As expected, the viability of all models was 100% for the 0 Gy condition. However, a spectrum of viability was observed when the models were exposed to different radiation levels. For instance, at the highest level of radiation, viability ranged from about 15% to 100%.
Overall, the Figure 2 graph depicts the most sensitive model on the left (i.e., OV5296B) and the most insensitive model on the far right (i.e., OV5294B). This heterogeneous response profile aligns with the diversity in radiotherapy responses observed in real-world patient populations.
Figure 2: Viability analysis after exposing 12 PDO models to different levels of radiation.
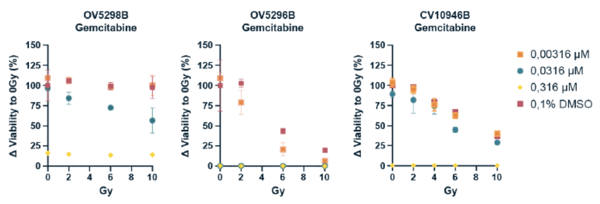
Subsequently, the synergistic effects of chemoradiotherapy in combination with gemcitabine, a known radiosensitizer drug, was tested in the most sensitive and insensitive models (i.e., the two ovarian tumor organoid models OV5298B & OV5296B) plus a model with moderate sensitivity (i.e., the cervical tumor organoid model CV10946B). As shown in Figure 3, The results of this analysis demonstrate that gemcitabine increased the radiosensitivity of all three tumor organoid models, irrespective of their baseline radiosensitivity.
Figure 3: Known radiosensitizing drug gemcitabine increases radiosensitivity of both sensitive and insensitive organoid models. CTG assay was used for this study, and values are represented as relative viability compared to solvent control at 0 Gy (error bars represent SD; n=2).
Conclusion
While radiotherapy is an important tool in the cancer treatment armamentarium, there remains ample opportunity to increase its safety and efficacy. Clinically predictive PDOs, which are amenable to HTS assays, are valuable models that can be used to discover novel radiosensitizers, both for existing SoC drugs or novel compounds.
Simplify your model selection with collated mutational and gene expression profiles for tumor organoid models with this searchable organoid biobank databaseof PDX-derived organoid (PDXO) tumor models and patient-derived organoids (PDO) organoid models.
Cite this Article
Baillargeon, M., (2023) Unlocking the Potential of Radiosensitizers with Patient-derived Tumor Organoids - Crown Bioscience. https://blog.crownbio.com/unlocking-the-potential-of-radiosensitizers
Antibody-drug conjugates (ADCs) are among the most exciting advances in target cancer therapy. They combine the specificity of monoclonal antibodies w…
Highly targeted antibody-drug conjugates (ADCs) combine an antibody with a cytotoxic payload, covalently attached via a chemical linker. These “biolog…
Antibody-drug conjugates (ADCs) represent a cutting-edge advance in cancer therapy. These targeted agents combine a monoclonal antibody and a cytotoxi…