 Explore how to use tumor organoids for immuno-oncology applications, including immunotherapy assessment through co-cultures with autologous and non-autologous immune cells.
Explore how to use tumor organoids for immuno-oncology applications, including immunotherapy assessment through co-cultures with autologous and non-autologous immune cells.
Challenges in Immunotherapy Drug Development
It’s well known that in vitro testing of cancer immunotherapies is challenging. This is due to I/O agents needing complex and dynamic interactions between the tumor and immune system that are only fully recapitulated in vivo.
However, available in vivo I/O models are also far from perfect. Current immuno-oncology models share common challenges, including:
- Species specificity: although homograft models feature a competent immune system they can only be used to evaluate cross-reactive or surrogate agents
- The complexity of humanized systems, which results in high developmental costs and timelines
- Graft-versus-host disease which limits the experimental window
- Donor-to-donor variability which can complicate data interpretation
- Partial or inefficient reconstitution of the immune system, which limits the applicability of I/O models to agents targeting non-reconstituted components
Using Organoid Co-Cultures for I/O Applications
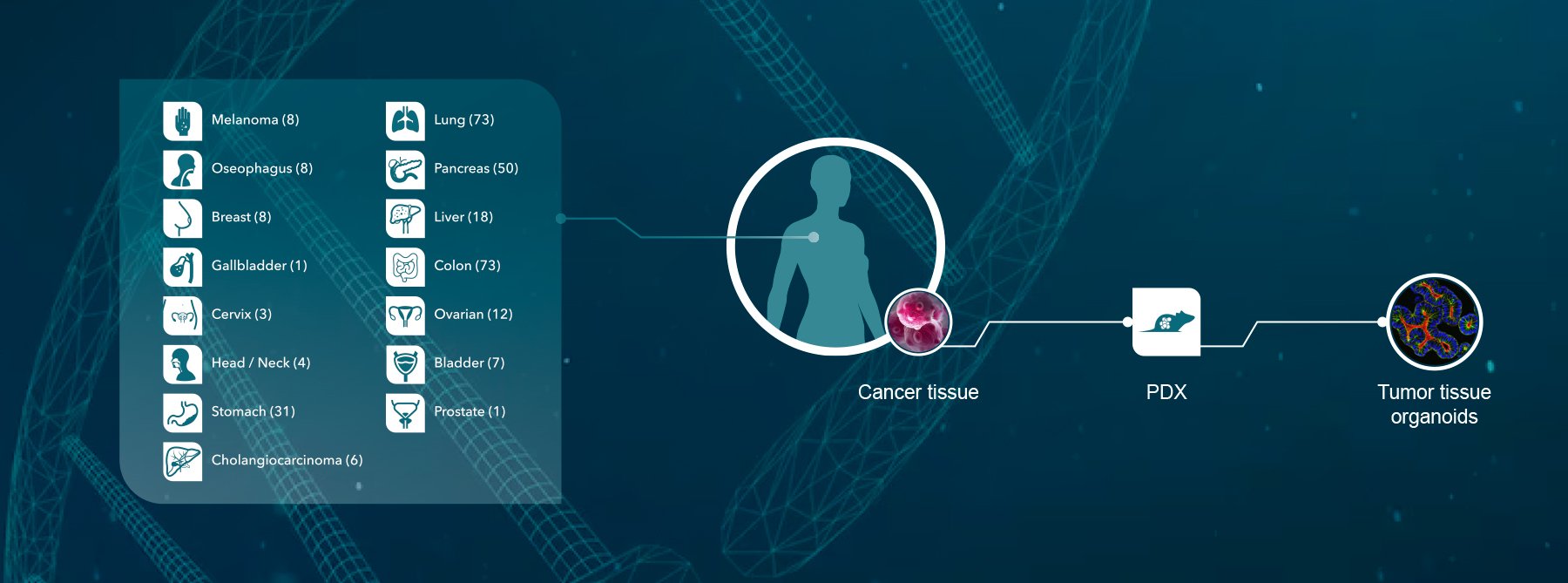
A new platform that may offer hope in using patient-derived models for in vitro immunotherapy assessment is tumor organoids, which are already revolutionizing the assessment of non I/O agents. These innovative patient-derived 3D models provide clinical relevance, population diversity, and patient-response predictivity.
So far, the main challenges in modeling immunotherapy response in vitro have been:
- The limited availability of patient material to test in co-culture systems
- The lack of antitumor reactivity of autologous immune cells.
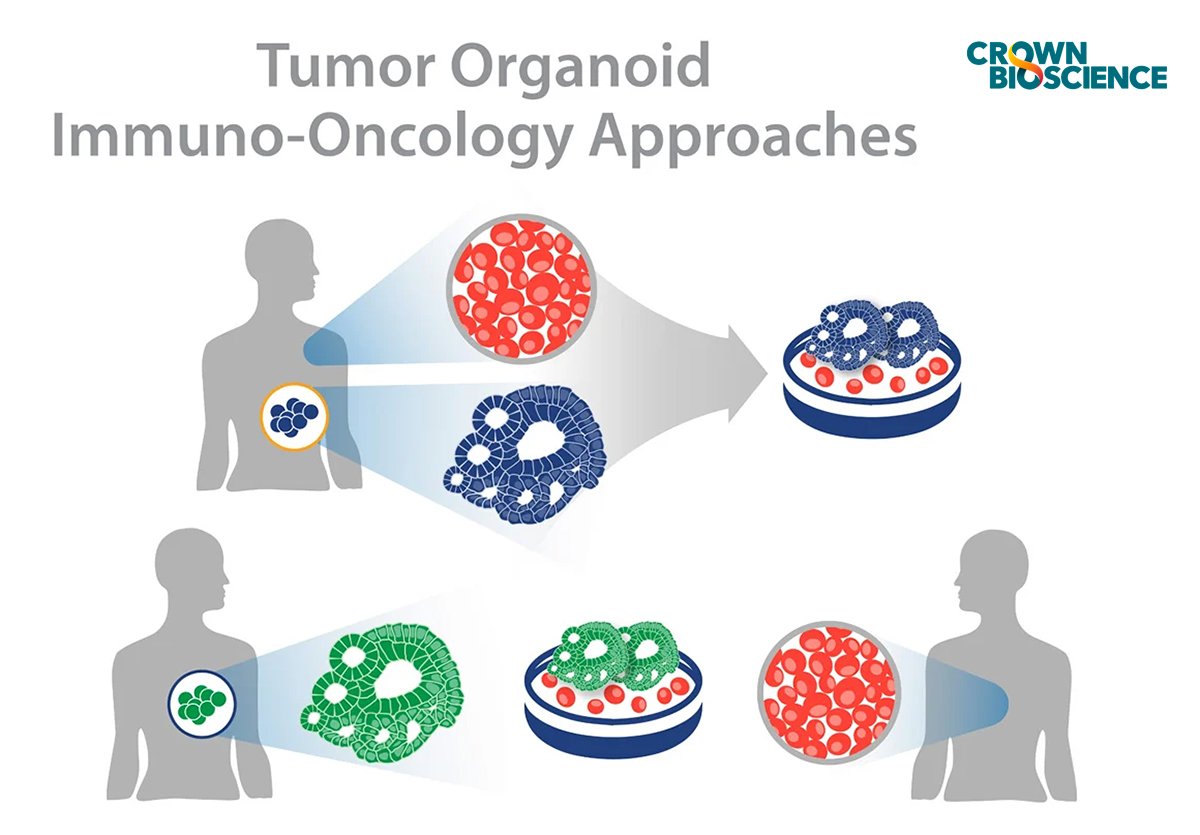
Tumor organoids are helping to overcome these issues. They are used in co-cultures with either autologous or non-autologous immune cells, to provide a patient-relevant in vitro platform for immunotherapy development.
The Benefits of Tumor Organoid and Immune Cell Co-Cultures
The benefit of in vitro tumor organoids for immuno-oncology applications is the enhanced clinical relevance of tumor organoids compared to cancer cell lines. The 3D architecture and spatial arrangement of multiple cell lineages results in the formation of mini-organs that recapitulate the genomic, morphological, and physiological features of the original tumor. This increased relevance helps produce more accurate efficacy and potency data for I/O agents, identify mechanisms of resistance or understand treatment failures, and model population diversity/heterogeneity.
The in vitro nature of organoid co-culture platforms also makes them more scalable than in vivo models, meaning multiple agents and donor/model combinations can be tested at the same time. Another benefit is that healthy organoids are also available or can be developed simultaneously to evaluate any potential off-target effects on human tissues in parallel, which is not possible with in vivo models.
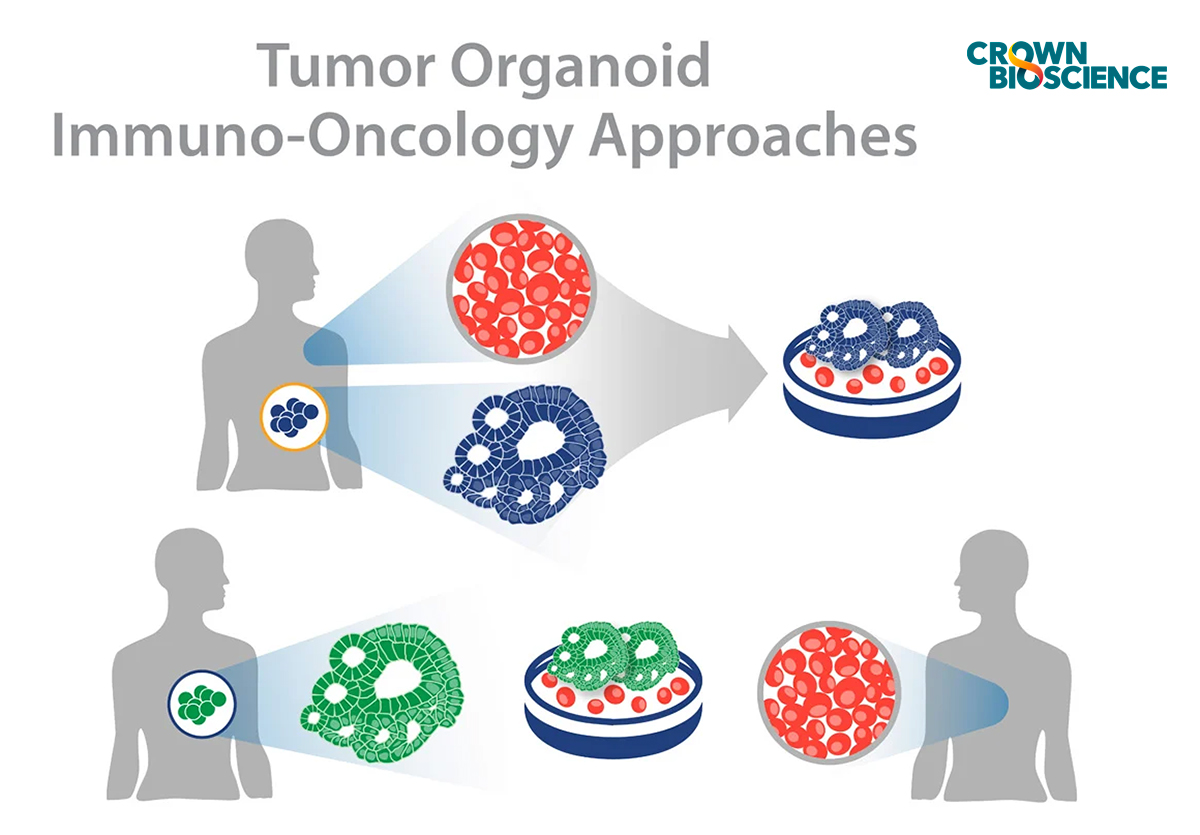
Tumor Organoid and Autologous Immune Cell Co-Cultures
This experimental approach involves combining immune cells and tumor organoids which are developed from the same patient (autologous). This co-culture system was published by Dijkstra et al., who evaluated T cell-specific responses against CRC and NSCLC organoids.
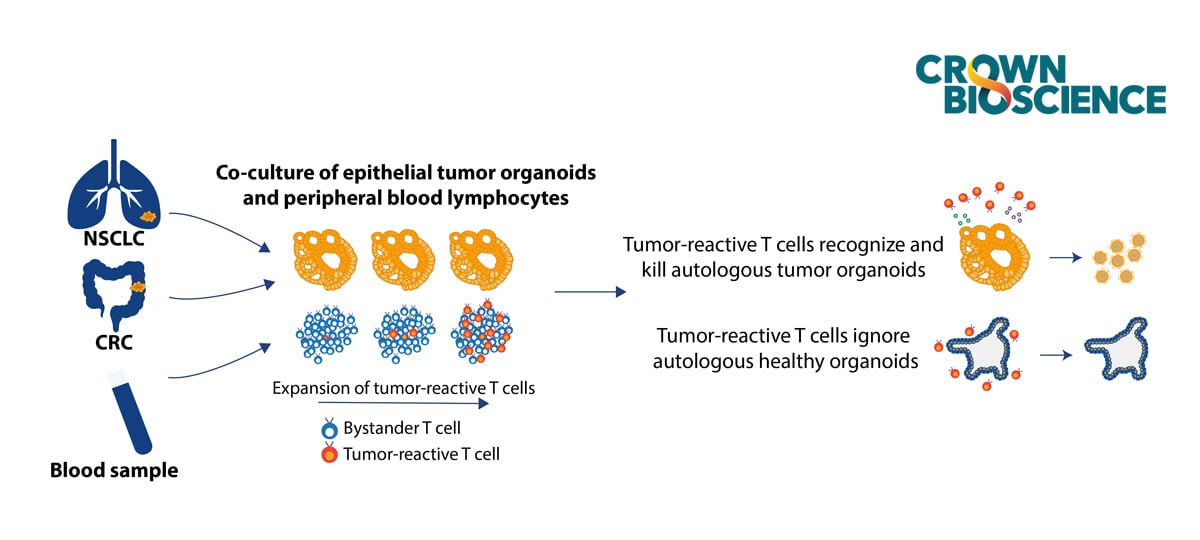
Strong tumor reactivity was seen after two weeks of tumor organoid co-culture with autologous PBMCs, measured by IFNγ secretion and CD107a upregulation in CD8+ T cells. These responses were confirmed to be tumor specific, as T cell reactivity was not detected in co-cultures with organoids derived from normal colon or lung tissue. Morphological and molecular analyses also indicated that the expanded autologous reactive T cells efficiently killed tumor organoids.
Challenges of Tumor Organoid and Autologous Immune Cell Co-Culture
Autologous PBMC and tumor organoid co-cultures are still highly experimental, at the research stage of development. There are some well-recognized challenges associated with this approach, including:
- Limited volume of blood from donor cancer patients
- Lack of tumor-reactive T cells among PBMC from most donor patients
- Limited scalability for drug development applications
Tumor Organoid and Non-Autologous Immune Cell Co-Cultures
A more feasible approach for immuno-oncology drug development is the use of organoid and non-autologous immune cell co-cultures which overcome some of the challenges discussed above. Non-autologous immune cells are much more readily available from healthy donors. Here, rather than using matched organoid and immune cells, the organoid or immune cells are selected based on different criteria.
- Organoids are selected based on the gene or protein expression profile of a target of interest or mutational burden
- Multiple non-autologous immune cells donors can be selected or different immune cells isolated
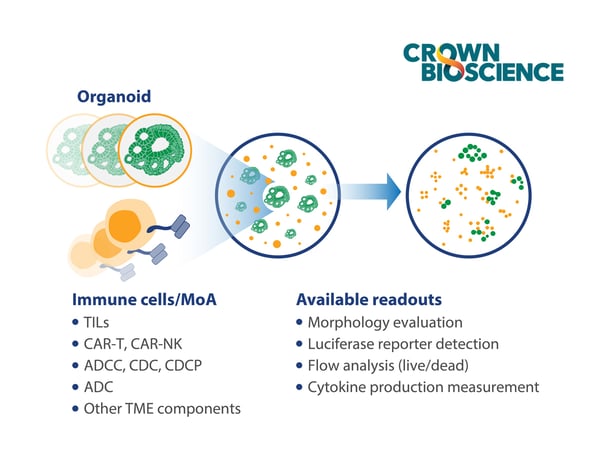
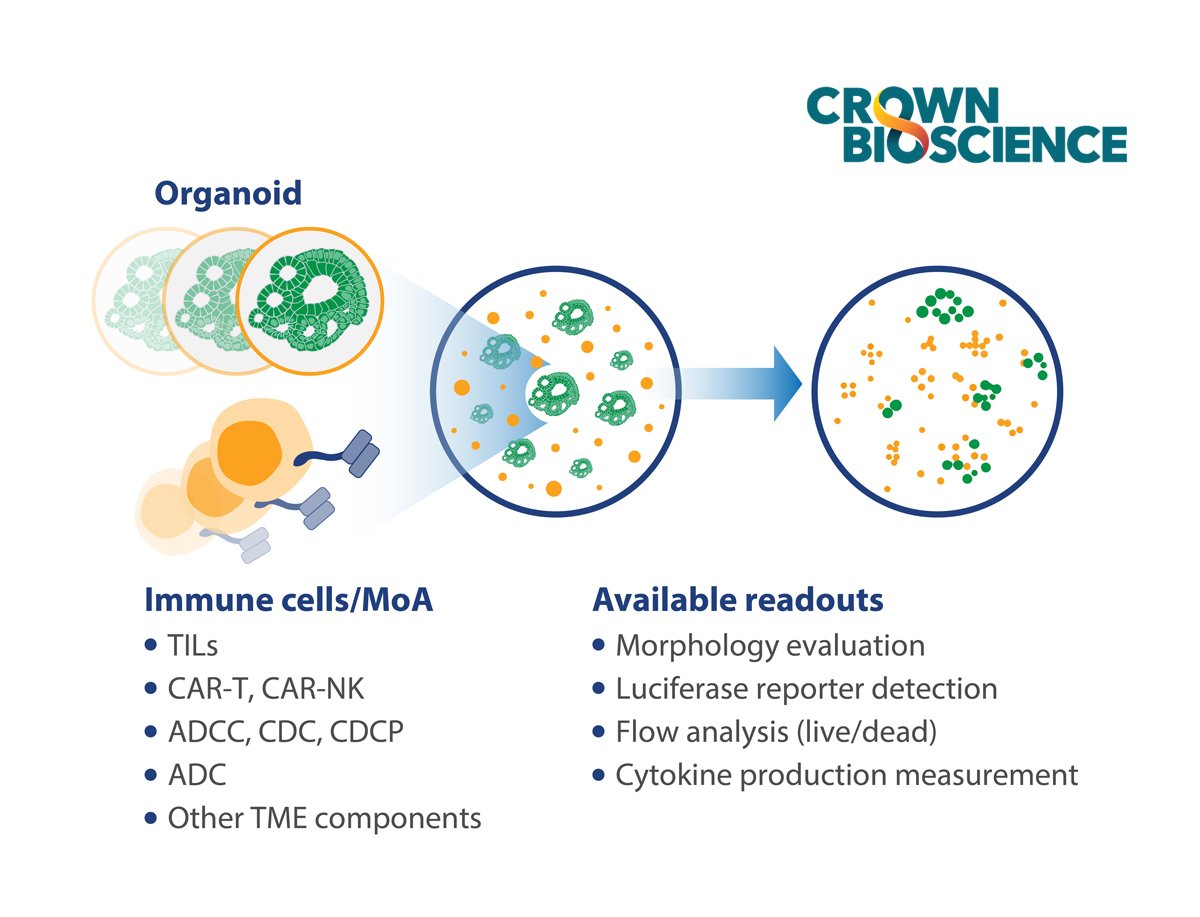
Tumor organoid and non-autologous immune cell co-culture platforms are used to assess:
- Tumor organoid killing by allogeneic T cells to evaluate the potency of immunotherapy agents
- Tumor organoid killing and tumor reactivity of CAR-T and TCR T cells
- Tumor organoid killing by ADCC (NK) and ADCP (macrophages)
 .
.
Challenges of Tumor Organoid and Non-Autologous Immune Cell Co-Culture
There are still some challenges associated with co-culturing organoids with non-autologous immune cells. These co-cultures can’t be used to test tumor antigen specificity. Organoid co-culture with non-autologous T cells tests the allogenic T cell response/killing of tumor organoids and measures the potency of immune checkpoint inhibitors. However, in the clinical setting, checkpoint inhibitors are aimed at improving T cell response to specific tumor antigens, instead of eliciting allogenic T cell responses. Further development of the organoid and non-autologous immune cell platform should allow the testing of tumor antigen specific T cell reactivity.
Engineering Tumor Organoids to Develop Unique New Immunotherapy Models
Another distinct advantage of tumor organoids for immuno-oncology applications, relative to in vivo models, is that they can be engineered to establish new immunotherapy models, such as by expressing specific CAR-T targets of choice. These models can also be modified to express luciferase or fluorescence reporters which allow the detection of tumor organoid killing via imaging.
Conclusion
Using tumor organoids for immuno-oncology applications offers researchers an attractive additional preclinical option for modeling the complexities of tumors in vitro for I/O drug development. While tumor organoid and autologous immune cell co-cultures are still in their infancy, new platforms combining tumor organoids and non-autologous immune cells are available for scalable immuno-oncology drug development applications. Using this approach allows better recapitulation of individual patients and produces more clinically relevant results.