Clinically-relevant prostate cancer patient-derived xenograft (PDX) models are notoriously hard to generate. Here we look at the challenges in developing prostate cancer PDX and review the characterization of some newly developed models.
Developing prostate cancer PDX is more difficult than for other indications. A well-known online resource for locating PDX currently contains only two prostate cancer models - and genomic and treatment data are only available for one of them.
Creating prostate cancer PDX is time consuming and labor intensive, with issues around both generation and propagation. Original tumor samples from the clinic are usually quite small, with limited tissue available, which often results in low take rates.
Growth rates of prostate cancer PDX are also slow, needing many months to generate models. Overall, this has left us with a lot fewer PDX models available than for other indications.
Propagation is also a problem once models have been established. There’s variation in how well models expand. Some may expand well, with something like a 1:5 ratio. Other models prove more challenging, providing limited passage donor material. This leads to poor expansion levels, which in turn impacts on how many models are banked and can be resuscitated.
How Can These Challenges be Overcome?
There isn’t really a magic trick to successfully creating prostate cancer PDX. Developing these models takes persistence and long-term resource commitments to overcome their low take rates and bank enough models.
PDX Model Success Factors
There are a few factors which can influence success when developing PDX prostate cancer models:
Engraftment site has been widely discussed, with subrenal capsule grafting potentially providing higher take rates than subcutaneous models, especially for less advanced cancers.
Mouse species could also be important, with a host needed which allows good engraftment rates from both localized and advanced disease e.g. NSG™.
There’s also the potential to add testosterone pellets at the time of tissue implantation.
New Panel of Prostate Cancer PDX Available
Despite the difficulties, prostate cancer PDX are available for translational preclinical studies, including a newly developed panel of three models.
This includes two castrate-resistant prostate cancer (CRPC) models and a third derived from a hormone responsive patient.
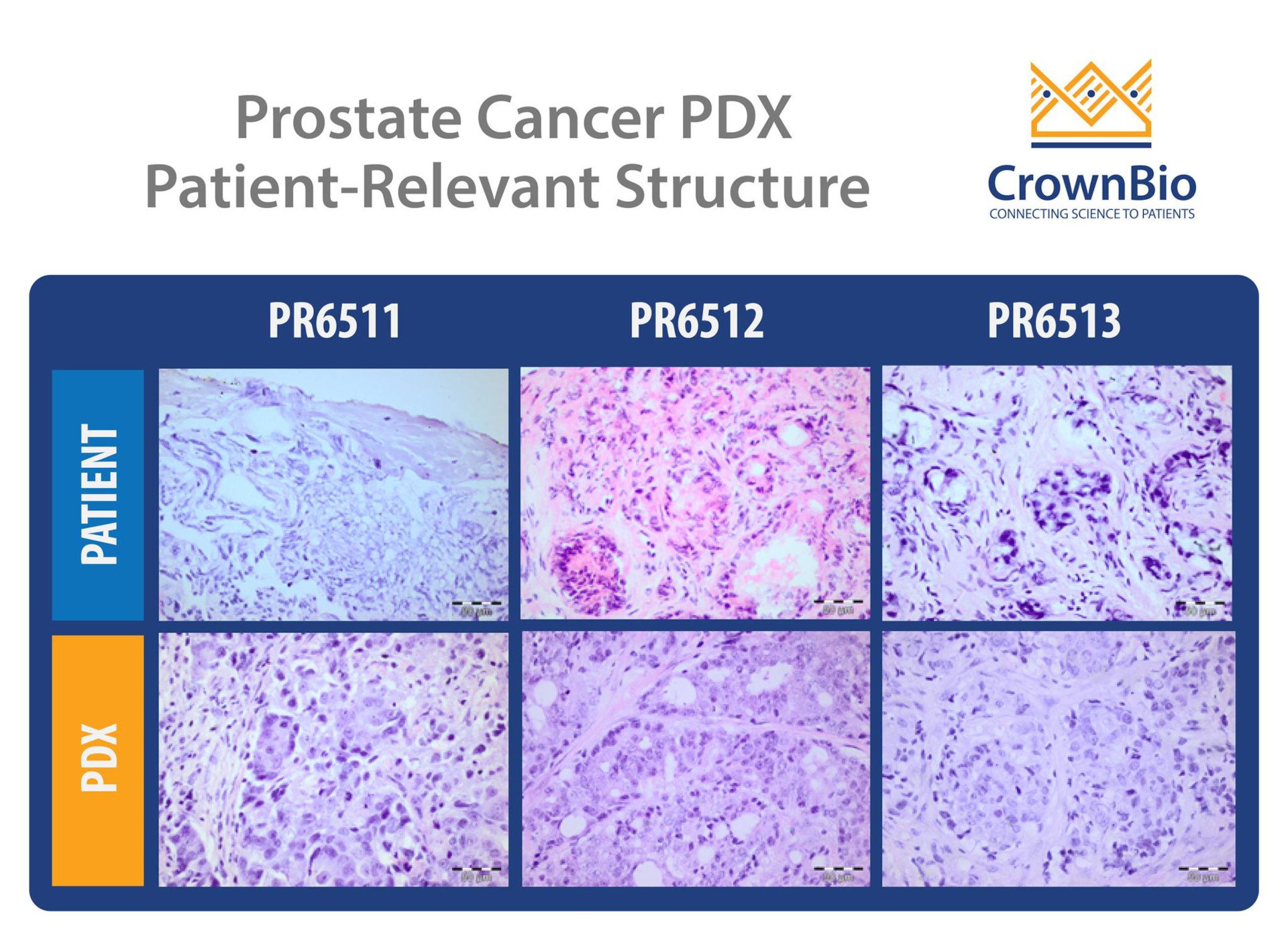
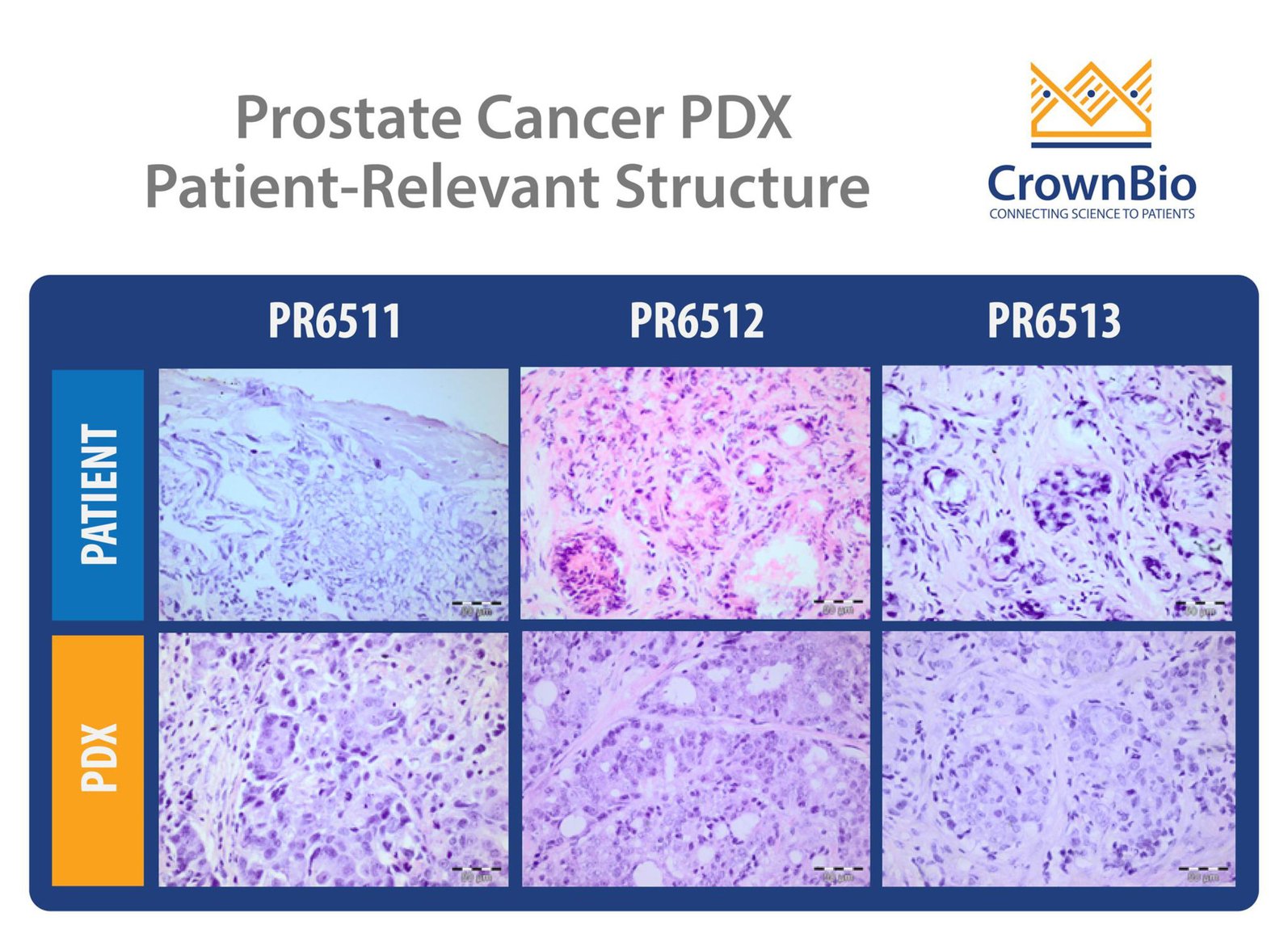
Prostate Cancer PDX Characterization and Validation
Histological analysis of all three models shows that they retain the structure of the matched original patient specimens. Both CRPC models have high KLK3 (PSA) expression levels, confirmed by RNA sequencing, which also detected the clinically relevant TMPRSS-ETS fusion in one model.
The two CRPC models have also been characterized by IHC to confirm their prostate adenocarcinoma diagnosis, and validated through treatment with standard of care chemotherapy (docetaxel) and hormonal agents (enzalutamide and abiraterone). The PDX have different responses to treatment, providing varying models as needed for preclinical studies.
Improved Preclinical Predictability with PDX Models
With know-how and perseverance, PDX models can be created even for difficult indications such as prostate cancer. As PDX provide the most predictive model for preclinical efficacy studies, this new panel of prostate cancer PDX will almost certainly improve clinical success rates for novel prostate cancer agents.
The integration of patient tumor samples and mass spectrometry is reshaping the landscape of cancer research and precision medicine. As researchers an…
Learn more about pancreatic cancer -- its associated risk factors, diagnosis, treatment and outcomes -- and current research into this understudied di…
Prostate cancer is a particularly difficult cancer type to model for preclinical research. Why are prostate cancer models so challenging, and how can …