The need for more clinically relevant preclinical models has been identified as one of the areas that can help reduce the high attrition rate observed for anticancer drugs. Better models, such as Hubrecht Organoid Technology (HUB) tumor organoids, can drive better decisions in drug discovery by identifying agents that will have the best chances of succeeding in clinical trials. In this post we explore the value of “living” tumor organoid biobanks for identifying anticancer agents with improved clinical relevance.
What are Tumor Organoids?
3D in vitro organoids have emerged as powerful predictive tools for many research applications to study not only normal developmental processes, but also mechanisms of disease such as cancer. In short, organoids are microscopic self-organizing 3D structures grown from adult stem cells. These “mini-organs” recapitulate the key phenotypic and genetic properties of the original source, making them highly patient-relevant, and having improved clinical relevance.
Optimized HUB protocols have been established to develop models from both normal and diseased tissue, including tumor tissue. Similar to PDX models, 3D in vitro tumor organoid models can be generated directly from patient tissue i.e. patient-derived organoids (PDOs) or from patient tissue expanded in mice as patient-derived xenograft organoids (PDXs/ PDXOs), and these models represent an alternative to working with primary patient cells.
Similar to their normal/healthy counterparts, tumor organoids highly recapitulate features of the parental tumor from which they were derived, including histopathology, genetic/epigenetic profiles, and even drug sensitivities. Tumor organoids are also scalable and they are genetically and phenotypically stable, even after long-term culturing and cryopreservation. Thus, tumor organoids result in highly reproducible results compared with data obtained from primary models, and since organoids preserve many of the key features of the original tumor, matched in vivo models can be generated to provide a transition from early in vitro studies to late-phase animal-based validation studies.
Collectively, these desirable features have made tumor organoids particularly valuable for identifying anticancer agents with improved clinical relevance. As explained in the next section, the availability of “living” tumor organoid biobanks means that these models can be used to support large-scale studies and ensure availability for repeat studies, especially true in cases where patient material is limited, while capturing the heterogeneity observed in patient populations because cancer is not a single disease.
Advantages of “Living” Organoid Biobanks
Tumor biobanks have long been used to store large collections of highly annotated human cancers, and these have been an important resource for researchers. However, the methods through which these samples are processed and stored often limits their use for large-scale in vitro screening studies.
In contrast, by using optimal cryopreservation techniques, “living” biobanks of organoids have been successfully generated using healthy tissue (for example see here) and tumor tissue from either PDX models or from primary patient samples collected directly from the clinic (resulting in biobanks of PDXOs and PDOs, respectively). Such tumor organoids can be used to generate living biobanks since they can be cryopreserved, thawed and expanded as needed (similar to cell lines), while retaining their key genetic and phenotypic features of their matched patient tumors.
Living organoid biobanks have now been established for many solid tumor types. Crown Bioscience has developed our Organoid Models Database, an extensive searchable biobank consisting of 342 tumor organoid models derived from its collection of PDX models (i.e., PDXOs) with information on histopathology, IC50, genomic, and transcriptomic analysis data associated with drug response, and an additional 217 models from primary patient samples (i.e., PDOs). These models have varied indications with multiple models derived from over twenty organ and tissue types.
Such biobanks allow researchers to bring clinical trials into the lab, sometimes referred to as “clinical trials in a dish” to identify predictive biomarkers of response (based on genomic profiling), combine drug strategies (e.g., multiple dose ratios, combination effects), and test therapeutic windows with healthy controls. High-content imaging (HCI) and analysis (HCA) is also being employed in large-scale organoid screening studies to generate rich data on drug effects beyond viability.
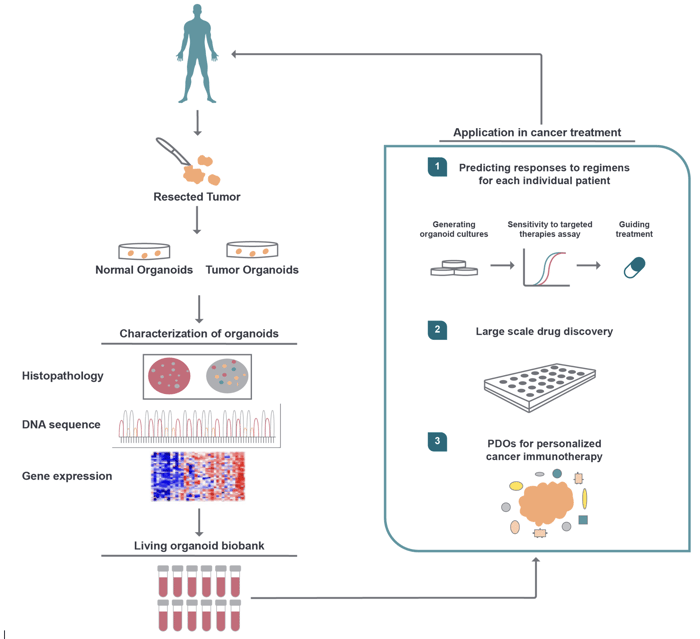
The following image depicts the development of a highly characterized living organoid biobank containing tumor organoids plus tissue-matched healthy organoids, plus their applications in cancer drug development.
From Zhou, Z. et al. Patient-Derived Organoids in Precision Medicine: Drug Screening, Organoid-on-a-Chip and Living Organoid Biobank. Front. Oncol., 30 December 2021. Available at: https://www.frontiersin.org/articles/10.3389/fonc.2021.762184/full. Used under Creative Commons Attribution 4.0 International License: https://creativecommons.org/licenses/by/4.0/.
Challenges of Using Tumor Organoids
While the benefits of using tumor organoids are clear, there remain some challenges that researchers should be aware of. For instance, not all tissues are amenable to organoid generation, and there exist different protocols being used to establish them depending on the tissue of origin and stem/progenitor cell compartment. Varying protocols may be a major contributing factor to the variability seen in organoid quality and success in establishing robust cultures, all of which can negatively affect data reproducibility. To get a sense of the issues limiting organoid researchers, check out this recent STAR Protocols online Q&A forum titled Organoids: questions and answers.
Reproducing the tumor microenvironment (TME) in organoid cultures is another challenge, albeit an increasing number of tumor organoid co-culture systems are now available to address this issue, and such systems have been successful in modeling immune cell migration and immunotherapy efficacy.
Conclusion
3D in vitro tumor organoids faithfully recapitulate the genomic, morphological, and pathophysiological characteristics of the original patient tumor. Further, they are more easily scalable than in vivo models, and they are genetically and phenotypically stable even after long-term culturing and cryopreservation. Living tumor organoid biobanks have now been developed to support large-scale studies. These organoid biobanks serve as living predictive models for cancer drug development. Now we can ensure availability, while capturing patient population heterogeneity (genomic, histopathological, and immunological diversity). These biobanks are being used to drive better decisions in drug discovery by identifying agents that have the best chances of succeeding in clinical trials.
To learn more about how Crown Bioscience can help progress your oncology drug development with 3D in vitro organoids, visit our organoids webpage.
Cite this Article
Pal, R., (2022) Organoid Biobanks: Living Predictive Models for Cancer Drug Development - Crown Bioscience. https://blog.crownbio.com/organoid-biobanks
Imagine standing on the brink of a breakthrough in cancer treatment, only to be halted by one daunting barrier: drug resistance. In this episode of Cr…
Oncology drug approvals in H1 2025 In the first half of 2025, the FDA’s Center for Drug Evaluation and Research (CDER) approved a total of 16 novel dr…
Often referred to as “magic bullets” or “biological missiles”, antibody-drug conjugates (ADCs) are one of the most promising advances in targeted canc…